
What IVDD Surgery Actually Involves
Dr. Alastair Greenway
MRCVS
Once surgery is on the table for a dog's disc problem, the questions tend to come in a rush. What actually happens in theatre? How long does the hospital stay last, how well does it work, and what could go wrong? The unfamiliar is what makes the decision feel so heavy, so this guide walks through IVDD surgery from start to finish, plainly and with the real figures attached. In my experience, knowing what is involved makes both the decision and the recovery a good deal less daunting.
First, the MRI
Surgery for a disc problem almost always begins with imaging, because the surgeon needs to know exactly which disc has herniated and precisely where, before operating. You cannot sensibly operate on a spine without a detailed map of the problem.
The imaging of choice is an MRI scan, which shows the spinal cord and the discs in fine detail and is the most accurate way to pinpoint a herniation; it is more sensitive than the alternatives such as CT, picking up disc herniations that other methods can miss. The scan is done under general anaesthetic, because the dog must be completely still, which is part of why imaging and surgery are often done in the same anaesthetic session. The dog is scanned, the problem is confirmed and located, and the surgery follows straight away, as our guide to seeing a neurologist explains. So the MRI is not a separate hurdle but the essential first step that makes precise surgery possible.
Inside the operation
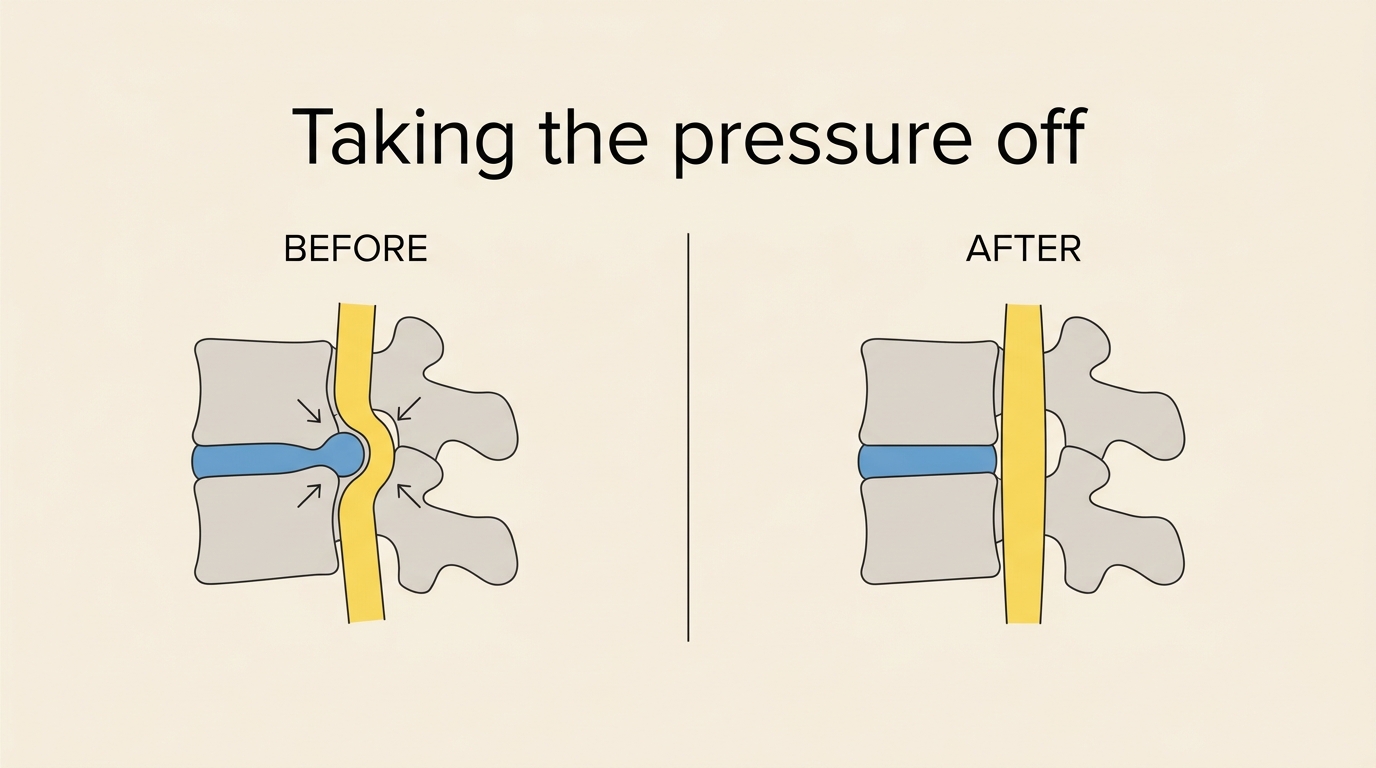
The aim of IVDD surgery is decompression: physically removing the herniated disc material that is pressing on the spinal cord, so the pressure comes off and the cord has the best chance to recover. The specific operation depends on where the disc is.
For a disc in the back, the thoracolumbar spine, the usual procedure is called a hemilaminectomy (or a mini-hemilaminectomy), in which the surgeon makes a small window in the bone of the vertebra to reach into the spinal canal and remove the herniated material pressing on the cord. For a disc in the neck, the cervical spine, the operation is usually different, a ventral slot, approached from underneath the neck, making a small opening to remove the offending disc material. Some surgeons also carry out fenestration during the same operation, removing the inner material from one or more discs to reduce the chance of a future herniation at those sites, which we come back to under risks and which our recurrence guide covers. In plain terms, then, the surgeon opens a small, carefully placed window in the bone, takes the pressure off the spinal cord by removing the herniated material, and, where appropriate, fenestrates to guard against a repeat. It is precise, well-established surgery performed by specialists.
The hospital stay
Surgery is not a same-day in-and-out affair; your dog will stay in the hospital for a period afterwards, typically a few days, for intensive nursing and monitoring. During this stay the team provides strong, appropriate pain relief, manages the bladder, which often needs help to empty in the early days after spinal surgery, watches closely for any complications, keeps the dog clean and comfortable, and begins the very first gentle physiotherapy. This intensive early care is an important part of why surgery is done in a specialist setting. When your dog comes home, the recovery continues with weeks of restricted activity and rehabilitation, much as for a conservatively managed dog, which our crate-rest and rehabilitation guides cover, so the hospital stay is the start of the recovery, not the end of the treatment.
How well it works
This is what owners most want to know, and the answer is encouraging, particularly for dogs that still have deep pain. The recovery rates depend heavily on how severely the spinal cord was affected before surgery, especially on deep pain perception, as our guides to the grades and to deep pain explain.
For dogs that have lost the ability to walk but still have deep pain present, the outlook with surgery is very good: pooled figures from across the research put recovery of the ability to walk at around ninety-three percent for these dogs. For dogs that have lost deep pain, the most severely affected, the outlook is more guarded but far from hopeless, with recovery after surgery pooled at around sixty-one percent. Neck surgery, the ventral slot, tends to do very well, with one study reporting recovery in around ninety-seven percent of dogs at a median of about a week. One crucial point to set expectations correctly: surgery removes the compression, but it does not instantly restore function. Recovery still takes time, often weeks, and still needs the rest and rehabilitation that follow, because the cord needs time to recover and the body needs to rebuild, as our rehabilitation roadmap describes. So surgery gives the cord its best chance, but the walking comes back gradually afterwards, not on the operating table.
Risks and complications
The risks belong here too, because no surgery is without them, though for most dogs the benefits outweigh them. There is the general risk of any anaesthetic and any surgery, including infection of the surgical wound. There is the possibility of an incomplete recovery, some dogs regain only partial function, and a few do not recover as hoped, particularly among the most severely affected. There is the chance of recurrence, another disc herniating at a different site in the future, which is part of why fenestration is sometimes done; reassuringly, recurrence at a disc that has been fenestrated is uncommon, reported at around two to three percent. Complication rates for the surgery itself are modest: one series of ventral slot operations reported an overall complication rate of around eleven percent.
One rare but grave complication belongs in any complete account: progressive myelomalacia, in which the spinal cord tissue itself breaks down. It affects only around two percent of dogs with thoracolumbar disc extrusion overall, though more, around fifteen percent, of the deep-pain-negative group, and it is usually fatal; it is part of why the most severely affected dogs are watched so carefully, and our guides on recovery red flags and on when surgery is not the right choice discuss it further. I include these not to frighten you but because a clear-eyed picture of surgery includes its risks alongside its genuinely good odds, and your neurology team will discuss the specific risks for your dog.
IVDD surgery means an MRI to map the problem, a precise decompression operation, a hemilaminectomy for the back or a ventral slot for the neck, to take the pressure off the spinal cord, a few days of intensive hospital care, and then weeks of rest and rehabilitation at home. It works well, especially for dogs that still have deep pain, around ninety-three percent of whom walk again, and still offers real hope, around sixty-one percent, even for those that have lost it. It carries the ordinary risks of surgery plus the rare grave one, all of which your team will talk through. It is a big step, but a well-understood one, and our guides to the cost, the recovery, and the rehabilitation pick up from the day you bring your dog home.
References
- da Costa RC, De Decker S, Lewis MJ, Volk H, The Canine Spinal Cord Injury Consortium (CANSORT-SCI). Diagnostic Imaging in Intervertebral Disc Disease. Frontiers in Veterinary Science, 2020;7:588338.
- Langerhuus L, Miles J. Proportion recovery and times to ambulation for non-ambulatory dogs with thoracolumbar disc extrusions treated with hemilaminectomy or conservative treatment: A systematic review and meta-analysis of case-series studies. The Veterinary Journal, 2017;220:7-16.
- Chang YP, Huang WH, Lua WZ, Wong W, Liu IH, Liu CH. Outcomes in Dogs with Multiple Sites of Cervical Intervertebral Disc Disease Treated with Single Ventral Slot Decompression. Veterinary Sciences, 2023;10(6):377.
- Aikawa T, Fujita H, Shibata M, Takahashi T. Recurrent Thoracolumbar Intervertebral Disc Extrusion after Hemilaminectomy and Concomitant Prophylactic Fenestration in 662 Chondrodystrophic Dogs. Veterinary Surgery, 2012;41(3):381-390.
- Dupont COC, Cherubini GB. Post-operative complications following cervical ventral slot in dogs: a retrospective review of the influence of prophylactic fenestration and chondrodystrophy in 593 cases. Frontiers in Veterinary Science, 2025;12:1616461.
- Balducci F, Canal S, Contiero B, Bernardini M. Prevalence and Risk Factors for Presumptive Ascending/Descending Myelomalacia in Dogs after Thoracolumbar Intervertebral Disk Herniation. Journal of Veterinary Internal Medicine, 2017;31(2):498-504.
Sister tool · Sightline
Track whether treatment is working
Sightline, a separate ConciergeVet tool, runs a short weekly check-in built on validated pain and mobility instruments, turns it into a single Sightline Score you can watch trend over weeks rather than judge on one bad day, and produces a report you can bring to your vet.
A written log, or our printable trackers, does much the same job.
See how Sightline tracks treatmentTrack the recovery, day by day
Recovery from a disc injury is all about the trend. Log the daily milestones through crate rest and rehab so you can see real progress, not just good and bad days.
Open the Recovery TrackerYou're not doing this alone
Compare treatment journeys and talk to owners managing IVDD. Free to join.
Join PetsLikeMine