
Surgery: The Decision-Making Framework
Claire Greenway
BVM&S MRCVS
Surgery tends to enter the picture in one of a few ways. Your vet has raised it as an option, your insurer has prompted a conversation about referral, or your own reading has led you to it. Whichever route you've taken to this page, there's a common misconception I want to clear up first, because it shapes how owners approach the whole decision.
No operation treats arthritis itself. Arthritis is a degenerative process; once cartilage is damaged, surgery can't restore it. What surgery does is address the underlying structural condition that's driving the arthritis, or salvage a joint that's become too damaged to function. The surgery is for the cause, not for the arthritis.
That distinction matters because it reframes the whole decision. Owners often ask "should I get the surgery?" as if it's a single question with a single answer. It isn't. The question is always: given the specific structural problem in my dog's joint, is surgery the right approach for them, at this stage of their disease, in their individual situation?
The answer varies enormously depending on which condition you're dealing with. Cruciate disease has different decision pathways from hip dysplasia, which has different pathways from elbow dysplasia, which has different pathways from end-stage joint degeneration. We have separate guides for each of these conditions where we have them, and more will be added as the content series develops.
This article covers something different. It's the universal framework that applies regardless of which specific condition is driving the surgical conversation. The decisions and considerations that affect every owner facing this conversation, irrespective of diagnosis. Whether to refer to a specialist, how to find the right surgeon, the cost reality, what to expect from anaesthesia and recovery, when to push for second opinions, and when surgery shouldn't be pursued.
Start with the diagnosis: is it specific and confirmed?
Before any surgical conversation makes sense, you need to know what you're treating.
"My dog has arthritis" is a description of degenerative change. It's the consequence, not the cause. For the surgical conversation to be meaningful, you need to know what's driving the arthritis. Is it cruciate ligament disease? Hip dysplasia? Elbow dysplasia? An old injury? End-stage degeneration with no specific lesion?
If your dog has had X-rays showing arthritis but no specific structural diagnosis, that's worth addressing before discussing surgery. Sometimes more detailed imaging (CT or MRI) is needed to characterise the underlying problem. Sometimes orthopaedic examination by a specialist is needed. Without a specific diagnosis, you're not in a position to evaluate surgical options.
If your dog has been diagnosed with a specific condition, the questions that follow are condition-specific. Hip dysplasia decisions are entirely different from cruciate decisions. The specifics matter.
A good vet should be able to tell you clearly what they think the underlying problem is. If they can't, more diagnostic work is the right next step, not surgery.
When surgical referral is genuinely indicated
Not every dog with a structural joint problem needs surgery. The decision depends on:
The specific condition. Some structural problems benefit dramatically from surgery (cruciate ligament rupture, severe hip dysplasia in young dogs, OCD lesions). Others may not need it at all if conservative management works (mild hip dysplasia, mild elbow dysplasia, low-grade patellar luxation).
The dog's age and stage of disease. A young dog with significant structural disease often has more to gain from surgical correction than an older dog with the same problem. Earlier intervention may prevent or slow the secondary arthritis. Once severe arthritis is established, surgery options shift from corrective procedures to salvage procedures.
The dog's response to conservative management. For some conditions, particularly those where surgical and non-surgical outcomes are similar, the question of whether to try conservative management first is reasonable. If pain is being well controlled, function is acceptable, and the dog is happy, surgery may not be needed despite a surgical option being available.
Comorbidities and overall health. Surgery on an otherwise healthy 5-year-old is different from surgery on a 12-year-old with kidney disease and cardiac concerns. The benefit-to-risk ratio shifts with age and concurrent disease.
Owner circumstances. Surgery requires post-operative rehabilitation, often weeks or months of restricted activity, frequently rehabilitation appointments, and significant financial commitment. If these can't be reliably delivered, the surgery may not produce its intended outcome.
In broad terms, surgical referral is worth seriously considering when:
- A specific structural condition has been diagnosed that's amenable to surgical correction
- The dog has years of life ahead of them where the benefit would compound
- Conservative management has been tried and is inadequate (where appropriate)
- The dog is healthy enough to tolerate surgery
- The owner is in a position to deliver post-operative care
- The cost is manageable for the family
Surgery is less appropriate when:
- The diagnosis is unclear
- Conservative management is working well and the dog is comfortable
- The dog has comorbidities making anaesthesia high-risk
- The expected lifespan is short relative to recovery time
- Post-operative care can't be delivered
- The owner has financial constraints that surgery would exceed
There's no universal right answer. The question is whether the surgery is right for the specific dog, the specific condition, and the specific situation.
Specialist referral vs general practice surgery

This is one of the most important questions owners face, and the right answer isn't always obvious.
Some orthopaedic procedures are routinely performed in general veterinary practice. Procedures like femoral head ostectomy (FHO), simpler fracture repairs, and certain straightforward operations are within the competence of experienced general practitioners.
More complex orthopaedic procedures should typically be referred to specialists. This includes:
- Cruciate stabilisation procedures (TPLO, TTA, etc.)
- Total hip replacement
- Triple pelvic osteotomy and similar pelvic procedures
- Arthroscopic surgery
- Complex fracture repair
- Elbow procedures (particularly minimally invasive ones)
- Joint replacement of any kind
- Salvage procedures requiring advanced techniques
The reason isn't snobbery. Specialist surgeons:
- Have completed additional postgraduate training (typically 3-4 years of residency)
- Hold recognised specialist qualifications (RCVS Recognised Specialist, EBVS European Specialist, ACVS American Specialist)
- Perform high volumes of these specific procedures (hundreds or thousands per year)
- Have access to specialised equipment
- Work with dedicated anaesthesia and nursing teams experienced in orthopaedic cases
- Have referral relationships with hydrotherapy and rehabilitation services for post-operative care
For procedures where outcomes are technique-dependent, surgeon experience matters significantly. Studies in human orthopaedics consistently show that volume of practice correlates with outcomes. The same applies in veterinary medicine.
If your vet has raised surgery as an option, ask directly: would this be done in this practice or referred to a specialist? Both answers can be appropriate, but knowing where the procedure would be performed informs everything else.
How to know if a surgeon is properly qualified
In the UK, look for:
RCVS Recognised Specialist in Small Animal Surgery (Orthopaedics). This is the UK specialist designation, requiring extensive postgraduate training and rigorous examination.
EBVS European Specialist in Small Animal Surgery. The European equivalent, also recognised in the UK.
Diplomate of ACVS (American College of Veterinary Surgeons). The American equivalent, sometimes held by UK-based surgeons trained in the US.
Diplomate of ECVS (European College of Veterinary Surgeons). Another European specialist designation.
RCVS Advanced Practitioner in Small Animal Orthopaedic Surgery. A step below full specialist status but indicates significant postgraduate training and experience.
What to be cautious about:
Vets describing themselves as "orthopaedic surgeons" or "specialists" without these specific qualifications. The terms aren't legally protected and some vets use them loosely. The qualifications above represent the recognised standards.
General practice vets performing complex specialist procedures occasionally. A vet who does two TPLOs per year is not the same as a specialist who does 200. Outcomes correlate with volume of practice.
Surgeons who pressure quick decisions without offering second opinions. Reputable surgeons welcome second opinions and aren't threatened by them.
Where the UK's orthopaedic referral centres are
Several centres in the UK have particular reputations for orthopaedic excellence:
Royal Veterinary College (RVC) at the Queen Mother Hospital for Animals near Potters Bar, Hertfordshire. University teaching hospital with multiple specialist surgeons. Strong research output and access to multidisciplinary expertise. The orthopaedic service is headed by recognised specialists with strong reputations.
Fitzpatrick Referrals in Eashing, Surrey. Founded by Professor Noel Fitzpatrick (well-known from the Supervet television series). One of the largest dedicated orthopaedic referral centres in the UK with a team of specialist surgeons and complete in-house rehabilitation services.
Animal Health Trust (AHT) historically based in Newmarket, though the organisation has changed structure in recent years.
London Vet Specialists offering comprehensive orthopaedic services in London.
Cambridge University Veterinary School. University teaching hospital with strong orthopaedic services.
Edinburgh University (Dick Vet) Veterinary Hospital. Strong orthopaedic team with research links.
Liverpool University Small Animal Teaching Hospital.
Glasgow University Small Animal Hospital.
Various private referral centres across the UK including Anderson Moores in Hampshire, Eastcott Veterinary Referrals in Wiltshire, Davies Veterinary Specialists in Hertfordshire, Wear Referrals in County Durham, North Downs Specialist Referrals in Surrey, and many others.
Don't be drawn solely by the most famous names. Excellent specialist orthopaedic surgery is performed at many centres across the UK. Your primary vet should be able to recommend appropriate options based on:
- Geographic accessibility (recovery means multiple appointments)
- Insurance coverage acceptance
- The specific procedure your dog needs
- Their professional relationships and clinical preferences
What it actually costs
UK orthopaedic surgery costs vary significantly by procedure, surgeon, and centre. Here are realistic ranges for the most common procedures at specialist centres (typically 2024-2026 pricing):
Cruciate stabilisation procedures:
- TPLO (Tibial Plateau Levelling Osteotomy): £5,500-7,000 per knee
- TTA (Tibial Tuberosity Advancement): £5,000-6,500 per knee
- Lateral suture techniques: £2,500-4,000 per knee
- Bilateral procedures (both knees): £8,000-12,000 typically
Hip procedures:
- Total hip replacement: £6,500-8,500 per hip
- Femoral head ostectomy (FHO): £2,500-4,500 (often performed in general practice for £1,500-2,500)
- Triple/double pelvic osteotomy (young dogs): £4,000-6,000
- Juvenile pubic symphysiodesis (very young dogs): £1,500-2,500
Elbow procedures:
- Arthroscopic procedures: £3,500-5,500
- Subtotal coronoid ostectomy: £4,000-6,000
- More complex elbow surgeries: £6,000-10,000
Other procedures:
- Patellar luxation surgery: £3,500-5,500
- OCD lesion arthroscopy: £3,000-5,000
- Complex fracture repair: £3,000-8,000
- Arthroscopic diagnostic procedures: £2,000-4,000
What's typically included:
- Pre-operative consultation
- Pre-operative imaging (often CT scan included)
- Anaesthesia and surgical fees
- Implants and surgical materials
- Post-operative hospitalisation (typically 1-3 nights)
- Initial follow-up appointments
- Discharge medications
What's typically not included:
- Post-operative rehabilitation (hydrotherapy, physiotherapy)
- Further investigation if complications arise
- Longer-term medications
- Treatment of unrelated conditions discovered during workup
A complete cruciate repair journey including surgery, rehabilitation, and aftercare typically costs £6,500-9,000 in total. A hip replacement journey is typically £7,500-10,500 per hip.
These are not small numbers. For multi-joint procedures or bilateral surgeries, total costs can reach £15,000-20,000 or more.
Insurance and pre-authorisation
Pet insurance covers most orthopaedic surgery in the UK, but the details matter enormously and getting this right before surgery is critical.
What to check before agreeing to surgery
Your policy's lifetime, per-condition, or annual limit. Lower-tier policies often have limits of £4,000-6,000 per condition per year. Higher-tier policies offer £15,000+ limits. For a £7,000 cruciate surgery on a lower-tier policy, you may need multiple policy years to fund the complete journey, which becomes complicated if the policy lapses or premiums rise dramatically.
Pre-existing condition exclusions. If your dog had lameness or specific signs before insurance started, the relevant joints may be excluded. Some insurers handle this strictly; others are more flexible.
Bilateral conditions. Many insurers have specific rules about bilateral problems (both knees, both hips, both elbows). Some treat the bilateral condition as one for cover purposes; others treat each side separately. This matters for cruciate disease particularly, where a significant proportion of dogs go on to rupture the cruciate on the other side within the following year or two.
Pre-authorisation requirements. Most major specialist centres can arrange pre-authorisation with insurers before surgery, which confirms cover and amounts. Some insurers require this; with others it's optional but recommended. Pre-authorisation gives you certainty about what's covered.
Direct claims processing. Many specialist centres have direct claims arrangements with major insurers. This means the insurance pays the centre directly rather than you paying upfront and claiming back. For surgeries costing thousands, this is enormously helpful for cash flow.
Conversations to have with the insurer
Before surgery, contact your insurer directly:
- Confirm what's covered for the specific procedure
- Confirm what limits apply
- Confirm whether pre-existing exclusions apply
- Confirm bilateral condition rules
- Request pre-authorisation if appropriate
- Confirm direct claim arrangement with the planned centre
Don't rely on your vet or the referral centre to manage the insurance side without your involvement. Mistakes happen, and they're costly. The insurance is your responsibility.
If you're uninsured
For uninsured owners facing major surgery costs, options include:
Payment plans. Many referral centres offer staged payment plans, particularly for procedures with predictable costs.
Care Credit or veterinary-specific financing. Various financing options exist for veterinary care, similar to consumer credit.
Charities. For owners in genuine financial hardship, charities including the PDSA, RSPCA, and Blue Cross may provide assistance. Eligibility criteria are strict and apply mainly to means-tested cases.
Conservative management as the realistic alternative. For some conditions, conservative management produces acceptable outcomes if surgery isn't financially feasible. This is a legitimate choice when surgery isn't accessible.
Don't agree to surgery you can't afford. The post-operative period requires ongoing financial commitment, and being unable to deliver care after surgery is worse than not having surgery at all.
Talking through the anaesthesia
Anaesthesia is one of the legitimate concerns owners raise about surgery, particularly for older dogs.
The reality is that modern veterinary anaesthesia is dramatically safer than it was twenty years ago. Specialist centres have:
- Dedicated veterinary anaesthetists (specialists in their own right)
- Comprehensive pre-anaesthetic workup including blood tests and often cardiac assessment
- Continuous monitoring during surgery (ECG, blood pressure, oxygen, capnography, temperature)
- Advanced support for older or compromised patients
- Experienced recovery nursing
The reference data on canine anaesthesia mortality comes from the Brodbelt et al. 2008 Confidential Enquiry into Perioperative Small Animal Fatalities (CEPSAF) study in Veterinary Anaesthesia and Analgesia. CEPSAF reported a perioperative death risk of around 0.17% across all dogs, dropping to roughly 0.05% (about 1 in 2,000) for healthy ASA grade 1-2 patients. For older or compromised dogs the risk is higher, but at modern specialist centres with appropriate workup it remains low.
What to discuss with the anaesthetist
For older dogs or dogs with concurrent disease:
- What pre-anaesthetic workup is recommended?
- Are there specific concerns about your dog's age or conditions?
- What modifications to standard anaesthesia protocols are appropriate?
- What's the realistic risk for your specific dog?
- What's the post-anaesthetic plan?
At specialist centres, you should have access to a dedicated veterinary anaesthetist for these conversations, not just the surgeon. The anaesthetist's expertise is specific to managing anaesthesia risk, which is different from the surgeon's expertise in the procedure itself.
When anaesthesia risk should change the decision
Age alone isn't a reason to avoid anaesthesia. Many 14-year-old dogs handle anaesthesia perfectly well at specialist centres with appropriate workup and management.
Specific reasons that should make you and your team think carefully:
- Severe cardiac disease that hasn't been adequately characterised
- Advanced kidney disease
- Significant respiratory disease (especially brachycephalic breeds)
- Concurrent conditions creating multiple anaesthetic concerns
- History of adverse anaesthesia reactions
For these situations, the decision becomes a careful balance of the surgery's potential benefit against the anaesthesia risk, the dog's expected remaining lifespan, and the availability of conservative alternatives.
The recovery commitment

This is where many surgical decisions become real. The surgery itself is one day. Recovery is months.
Typical post-operative requirements for major orthopaedic procedures:
Strict rest period. Often 4-8 weeks of severely restricted activity. Crate or small room confinement, only out for toileting on lead. No running, jumping, or playing.
Controlled exercise gradually. From around 4-6 weeks, structured lead walks beginning at 5 minutes twice daily, slowly increasing.
Rehabilitation appointments. Hydrotherapy and/or physiotherapy typically starting 2-6 weeks post-op depending on the procedure. Often weekly for several months.
Follow-up imaging. X-rays typically at 4-6 weeks and again at 3 months to confirm appropriate healing.
Activity modification long-term. Full return to previous activity levels typically at 4-6 months, sometimes longer.
Cone or surgical recovery suit. For the first 2 weeks to prevent licking at the wound. Genuinely difficult for some dogs and households.
Pain management. Comprehensive pain control for the first 2-4 weeks at minimum, often longer.
Frequent monitoring at home. Wound inspection, gait observation, medication administration, restricted activity supervision.
Gait observation in particular is harder than it sounds for the months of recovery that follow a major procedure. You're trying to compare how your dog is moving at week four to how they were moving at week one, and the eye isn't well suited to that. This is one of the use cases we built PAWSCHECK for. PAWSCHECK (pawscheck.co.uk) is a separate ConciergeVet tool that produces an objective AI gait analysis from a short smartphone video, reviewed by a UK RCVS vet, with the trajectory plotted over time so the recovery curve becomes visible.
I mention this because the broader principle stands regardless. A surgeon who's invested several thousand pounds and several months of recovery into your dog's joint wants reliable feedback on how the joint is performing, not just at the four-week check, but in the weeks between. Phone video to the surgical team, a structured written log, gait analysis: any of these is better than waiting for the next clinic appointment and trying to remember.
Can you deliver this? Truthfully?
For working households with limited supervision, dogs who genuinely can't be confined safely, families with young children who interact constantly with the dog, or dogs with significant separation anxiety, the practical reality of recovery can be harder than the surgery itself.
This is a legitimate factor in the decision. The best surgical technique fails if recovery can't be delivered. If you can't reliably provide the post-operative environment needed, surgery may not be the right choice even if it's clinically indicated.
When surgery should NOT be pursued
Surgery isn't always the right answer, even when it's technically possible. Situations where I'd recommend against it:
The diagnosis isn't clear. Operating on undiagnosed problems is a recipe for unhappy outcomes. Get the diagnosis right first.
Conservative management is working well. A comfortable, happy dog whose pain is being controlled effectively doesn't need surgery, even if a surgical option exists.
Comorbidities make the anaesthesia risk too high. Some dogs are genuinely too compromised to tolerate major surgery. Conservative management may be the right path for them.
Expected remaining lifespan is short. For a dog with a serious concurrent condition limiting their expected lifespan to weeks or months, major surgery with 3-6 month recovery may not deliver enough benefit.
Post-operative care can't be delivered. If you genuinely can't restrict your dog's activity for 2 months, can't deliver medications reliably, or can't transport them to rehabilitation appointments, the surgery's success will be compromised.
Cost would create genuine financial hardship. Don't make surgical decisions that will create serious financial problems. Conservative management is a legitimate alternative.
Quality of life is good enough. A dog who's comfortable, engaged, and enjoying their life on conservative management doesn't need surgery just because surgery is theoretically available.
Choosing not to pursue surgery is a valid decision. It's not giving up. It's recognising that for some dogs, in some situations, conservative management is the right path.
Second opinions
You're entitled to a second opinion. Reputable surgeons welcome them and aren't threatened by the request. If you're feeling uncertain about a recommendation, getting another specialist's view is reasonable.
When second opinions are particularly worth seeking:
- Significant cost decisions where you want to confirm the approach is necessary
- Cases where the clinical picture seems borderline (could go either way)
- Complex situations with multiple possible approaches
- Cases where you feel rushed in the original consultation
- Cases where the first surgeon seems dismissive of conservative alternatives
Second opinions don't have to be in person. Many specialists offer telemedicine consultations for case review. This is particularly useful when the original imaging and notes can be shared, allowing a remote assessment for a fraction of the cost of a full referral.
If two specialists offer different recommendations, that's information worth processing carefully. Sometimes there are genuinely two reasonable approaches. Sometimes one approach is clearly better. The disagreement itself is useful for clarifying the decision.
A practical framework for the decision
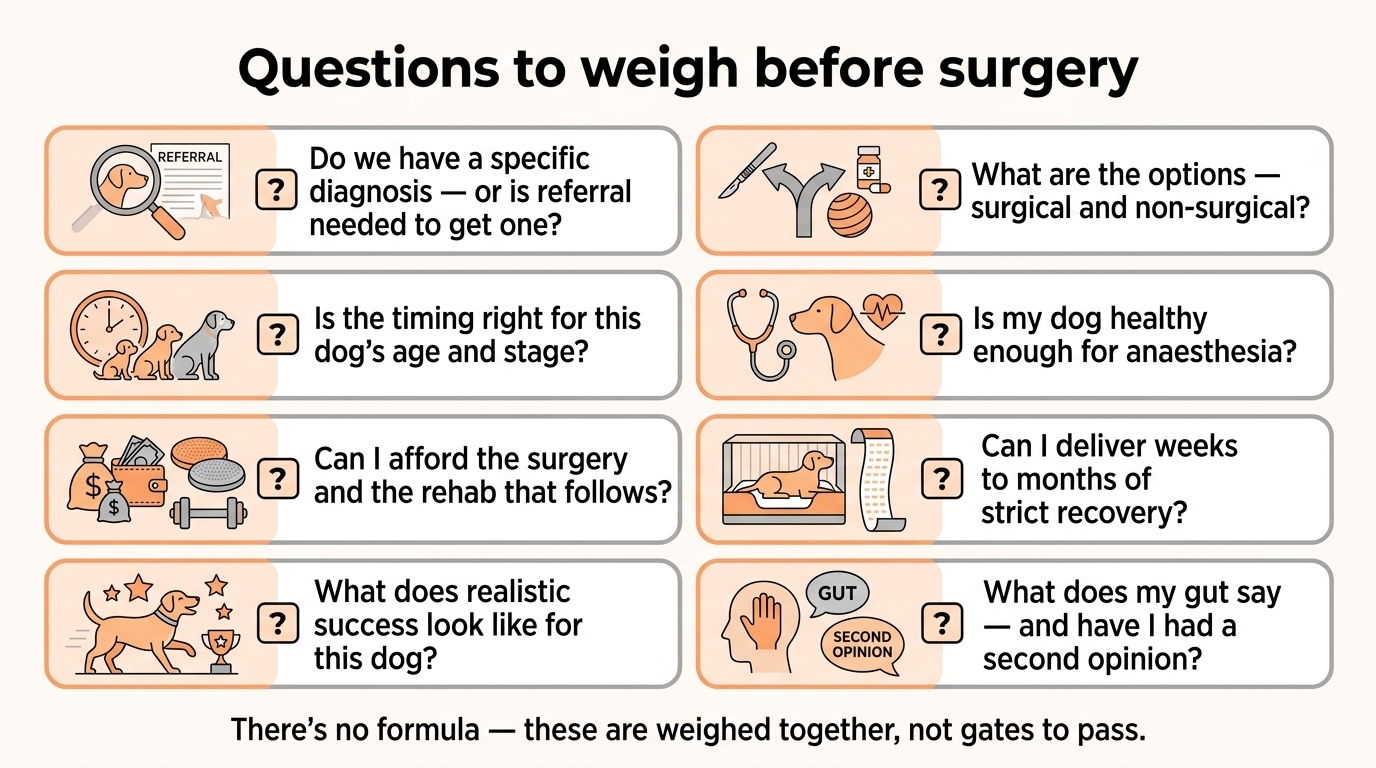
When facing a surgical decision, work through these questions:
-
Is the diagnosis clear? What specifically is wrong with the joint? What's the underlying structural problem?
-
What are the options? Surgical and non-surgical. What does each involve? What are the realistic outcomes?
-
Is the timing appropriate? Is this the right age and stage of disease for this intervention?
-
Is my dog healthy enough? What's the anaesthesia and surgical risk? Are there comorbidities that need addressing first?
-
Can I afford it? Both the procedure and the rehabilitation that follows. Including managing complications if they arise.
-
Can I deliver the recovery? Strict rest, controlled exercise, rehabilitation appointments, medication administration, for months.
-
What's the realistic expected outcome? What does success look like for this specific dog?
-
What does my gut tell me? Sometimes clinical analysis points one way but instinct points another. Both are worth weighing.
-
Have I had a second opinion if I'm uncertain?
-
Is this the right decision for this dog at this time?
Take the time to work through these properly. Major surgery isn't a decision to make in a single consultation. Take notes, go home, sleep on it, discuss it within the family, talk to other owners who've been through similar decisions.
The emotional dimension
I haven't said much about the emotional aspect yet, but it deserves explicit attention.
Major surgical decisions for a beloved dog are emotionally difficult. The fear of anaesthesia. The worry about complications. The cost stress. The recovery commitment. The uncertainty about whether you're making the right choice. The guilt about the question itself.
All of this is normal. None of it makes you a worse owner.
A few practical points on the emotional side:
Don't decide alone. Discuss the decision with family. With friends who know your dog. Frankly, with your vet. With other owners who've been through similar situations (PetsLikeMine community can be valuable here).
Don't decide in crisis. If you're feeling overwhelmed by a recent diagnosis, give yourself time before committing to a major surgical decision. Most orthopaedic surgery has flexibility on timing. A few weeks to think clearly is usually fine.
Acknowledge the uncertainty. No decision in medicine is risk-free, including the decision not to operate. Accept that you're making the best decision you can with the information available.
Forgive yourself for whatever you decide. Whatever you choose, with the information you have, with your best judgement, with love for your dog, it's a defensible decision. Don't carry guilt afterwards if outcomes don't match hopes.
A final thought

Surgery for your dog's underlying joint condition can be transformative. It can also be unnecessary, ill-advised, or beyond your circumstances to manage. Often it's somewhere between these extremes: a reasonable option with real benefits and real costs, requiring careful weighing in the specific context of your dog and your family.
The condition-specific questions (which cruciate technique, which type of hip surgery, which elbow procedure) belong in dedicated guides for those specific situations, some of which we have, others which we'll develop as the content series grows.
If your dog has been raised as a potential surgical candidate, give the decision the time and thought it deserves. Discuss it thoroughly with your primary vet. Get specialist input where appropriate. Understand the costs, the recovery, the risks, and the expected outcomes. Ask the questions that matter. Get a second opinion if you need one. Then make the decision that's right for your dog, your family, and your circumstances.
References
Sister tool · Sightline
Track whether treatment is working
Sightline, a separate ConciergeVet tool, runs a short weekly check-in built on validated pain and mobility instruments, turns it into a single Sightline Score you can watch trend over weeks rather than judge on one bad day, and produces a report you can bring to your vet.
A written log, or our printable trackers, does much the same job.
See how Sightline tracks treatmentSee where your pet stands today
Tracking is the other half of managing arthritis. Take the 2-minute Mobility Check to see your pet's stage, then watch it shift as treatment takes effect.
Take the Mobility CheckYou're not doing this alone
Compare treatment journeys and talk to owners managing arthritis. Free to join.
Join PetsLikeMine