
Regenerative Medicine: Stem Cells, PRP, and Beyond
Dr. Alastair Greenway
MRCVS, 25 years clinical experience
Regenerative medicine for canine arthritis sits in an interesting position. The science is genuinely exciting, the early case reports include some remarkable transformations, and specialist centres are increasingly offering these treatments. The marketing around it, in some cases, is several steps ahead of the actual evidence base.
What I want to do here is give you a clear-eyed look at where regenerative medicine actually stands for dogs with arthritis. What stem cell therapy is, what platelet-rich plasma involves, what other emerging treatments are on the horizon, what the evidence supports today, what's still developmental, and what realistic expectations should be. By the end, you'll be equipped to engage thoughtfully with these treatments rather than being swept along by marketing or dismissed by reflexive scepticism.
Two things I want to be transparent about from the start.
First, the field is moving fast. What's accurate in early 2026 may need updating by 2027 or 2028 as more evidence accumulates. Where the picture is genuinely uncertain, I'll say so rather than pretend to certainty I don't have.
Second, regenerative medicine has been overhyped in both human and veterinary contexts in ways that have damaged patient interests. Owners have spent significant money on treatments that delivered less than promised. I want to be clear-eyed about both the genuine promise and the limitations, because owners deserve straight information when major financial decisions are involved.
These treatments aren't magic, but they're not nothing either. The truth is somewhere in the middle. Let's work out where.
What "regenerative medicine" actually means
The term covers a few different approaches that share a common idea: using biological agents to influence the body's own healing and repair processes rather than just managing symptoms.
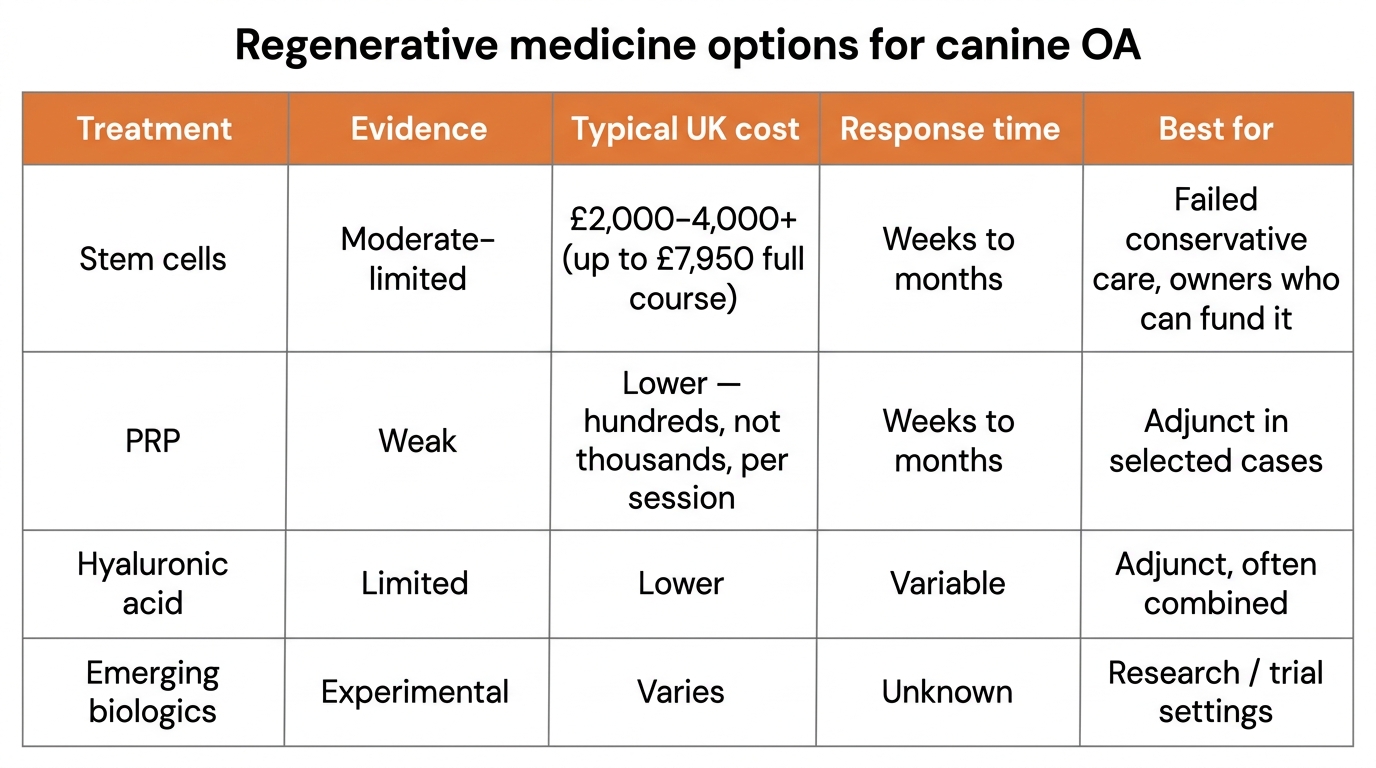
The main categories relevant to canine arthritis are:
Stem cell therapy. Using mesenchymal stem cells (MSCs), typically harvested from the dog's own fat or bone marrow, to influence joint inflammation and theoretically support tissue repair.
Platelet-rich plasma (PRP). Concentrated platelets from the dog's own blood, containing growth factors that may reduce inflammation and support tissue healing.
Hyaluronic acid injections. Synthetic or biological versions of the natural lubricating molecule in joint fluid, injected to improve joint function.
Emerging biologics. Monoclonal antibodies beyond Librela, gene therapy approaches, and other targeted therapies in various stages of development.
Each of these has a different evidence base, a different mechanism, a different cost, and a different appropriate use. Lumping them all together as "regenerative medicine" can obscure significant differences, so I'll address each separately.
Stem cell therapy
Stem cell therapy is the most discussed regenerative approach in canine arthritis. It's also the one with the most varied evidence base and the most variable marketing.
What it actually is
Stem cells are cells with the capacity to develop into different cell types and to influence the behaviour of other cells around them. Mesenchymal stem cells (MSCs) are a specific type of stem cell that can be derived from various tissues including bone marrow, fat (adipose tissue), and umbilical cord material.
For canine arthritis, the typical approach is autologous adipose-derived stem cell therapy. This involves:
- Surgical removal of a small amount of fat tissue from the dog (typically from the falciform ligament or subcutaneous fat)
- Laboratory processing to isolate and concentrate the mesenchymal stem cells
- Injection of the prepared cells into the affected joint(s)
Some centres also use bone marrow as the source. A few use allogeneic (donor) stem cells rather than the dog's own cells, though autologous treatment is more common.
How it's claimed to work
The proposed mechanisms include:
Immunomodulation. MSCs release signalling molecules that modulate the immune response in the joint, reducing the chronic inflammatory state of arthritis.
Trophic effects. MSCs release growth factors and cytokines that may support the surrounding cells and tissues, potentially slowing degeneration.
Cartilage-supportive effects. The theoretical hope is that MSCs may support cartilage health, though the evidence for actual cartilage regeneration in clinical settings remains limited.
Anti-inflammatory effects. Reduction of pro-inflammatory cytokines that drive ongoing joint damage.
One point worth being clear about: the "stem cells become cartilage" narrative that some marketing promotes is largely not what we believe is happening clinically. The benefits, where they occur, are more likely to come from the cells' immunomodulatory and trophic effects than from direct tissue regeneration.
Evidence, and how strong it really is
This is where the careful assessment matters.
A 2021 systematic review by Olsson and colleagues in Research in Veterinary Science examined six clinical trials of adipose-derived stem cells injected at the hip joint of dogs with osteoarthritis. All six reported significantly better outcomes (pain, function, hip OA evidence) with stem cell treatment. The authors also noted that the risk of bias was moderate-to-high across the included studies and that heterogeneity prevented a formal meta-analysis. So: consistent direction of effect, but with the caveats that the formal evidence base is small and the methodological quality is uneven.
A 2021 narrative review by Brondeel and colleagues in Frontiers in Veterinary Science assessed the broader stem cell literature in canine OA and concluded that studies generally show a tendency to improve lameness, joint pain, and range of motion, while noting significant variation in study design and incomplete data limiting evaluation of true efficacy.
A 2025 three-part review series by Halperin in Companion Animal (UK Vet) examined the clinical evidence for canine stem cell therapy in osteoarthritis. The series concluded that promising results exist in clinical trials but that standardisation of protocols and longer follow-up periods are still needed.
A fair summary of the current veterinary evidence: stem cell therapy for canine OA shows positive trends in clinical studies but the formal evidence base has significant limitations. Most studies are small. Follow-up periods are often short. Standardisation of cell preparation, dose, and treatment protocols varies between studies. Direct comparison with conservative management or other treatments is limited.
The human knee OA literature on MSC therapy is more mature but more contested than is sometimes presented. A 2025 systematic review and meta-analysis (Cao and colleagues, Stem Cell Research & Therapy, eight RCTs and 502 patients) reported significant improvements in WOMAC, VAS and KOOS scores at 6 and 12 months. A more rigorous, larger 2024 individual-participant-data meta-analysis (Sadeghirad and colleagues, Osteoarthritis and Cartilage, 16 trials and 807 patients, GRADE methodology) reached a much more cautious conclusion: that MSCs "probably provide little to no improvement in pain or physical function" in human knee OA. Both reviews are real, both pass peer review. The right reading is that the human evidence is genuinely contested, not settled in either direction.
The picture is encouraging but not yet definitive. Stem cell therapy may genuinely help some dogs with arthritis. It may help significantly. But the evidence supporting the strong claims sometimes made for it is weaker than the marketing suggests.
Realistic expectations
So what does "improvement" actually look like in stem cell therapy for canine OA?
Studies and clinical experience suggest that responding dogs typically show:
- Reduced lameness scores over weeks to months
- Improvement in owner-assessed pain and quality of life
- Better range of motion in affected joints
- Increased activity levels
- Sometimes reduction in pain medication requirements
What stem cell therapy does not appear to do, despite some marketing implications:
- Reverse established arthritis
- Restore damaged cartilage to normal
- Provide a one-time cure for chronic disease
The realistic position is that stem cell therapy can be a useful additional intervention for some dogs with arthritis, particularly those whose conservative management isn't providing adequate quality of life. It isn't a cure, and it isn't a replacement for the foundational interventions of pain control, weight management, exercise and environment.
Who might benefit
The dogs who appear most likely to benefit from stem cell therapy include:
Dogs with moderate to severe arthritis where conservative management is failing. Where pain medication, weight management, environmental modification, hydrotherapy, and other interventions aren't providing acceptable quality of life.
Dogs who can't take NSAIDs. Where pharmaceutical pain options are limited by kidney disease, liver disease, or intolerance.
Younger dogs with significant joint disease. Where slowing disease progression has more potential value over their remaining lifetime.
Dogs undergoing orthopaedic surgery. Where stem cells may support post-surgical recovery and joint health.
Dogs whose owners can afford the cost and understand that the response, if any, may take weeks to months to assess.
Less likely to benefit:
Dogs with very advanced end-stage arthritis. The theoretical regenerative effects can't restore tissue that's no longer there.
Dogs with primarily mechanical problems that surgery would address better.
Dogs whose conservative management is working well. The risk-benefit doesn't justify the cost when the foundation is already delivering acceptable outcomes.
Realistic UK costs
Stem cell therapy isn't cheap. UK pricing reflects the laboratory processing involved and the specialist nature of the centres offering it.
Initial treatment at UK specialist centres typically falls in the range of approximately £2,500-4,000, which usually includes the fat harvest procedure, cell processing, and injection into one or two joints. Some centres charge a smaller additional fee per extra joint treated at the same session.
Comprehensive programmes that include banked cells for future use and multiple planned treatments can run higher, sometimes £7,000-9,000+ for a full course at the more comprehensive providers.
Repeat treatments. Most centres offer banked cells for future use, but additional injections (often recommended at intervals of 6-12 months) incur additional costs.
Total cost over the lifetime of an arthritic dog can range from £3,000 to £10,000+ depending on the centre, the treatment plan, and how often retreatment is pursued. Pricing varies between centres and changes over time, so confirm specific costs directly with the provider before committing.
That's significant money. The clinical decision should involve realistic expectation-setting about what the treatment is likely to deliver for your individual dog.
Pet insurance considerations
Many pet insurance policies cover stem cell therapy when it's veterinary-administered and recommended for a covered condition. The specifics vary considerably between insurers and policy tiers.
Things to check before committing:
- Whether your policy covers regenerative medicine specifically
- What limits apply (some have sub-limits for these treatments)
- Whether pre-authorisation is required
- Whether the specific provider you're considering has direct claims arrangements
- Whether repeat treatments would also be covered
As with surgery, don't rely on the referral centre to manage the insurance side. Have the conversation with your insurer directly before committing.
Platelet-rich plasma (PRP)

PRP is the second main regenerative therapy used for canine arthritis. It's simpler than stem cell therapy, faster to deliver, and considerably cheaper. The evidence base, however, is currently weaker.
What it actually is
PRP involves taking a blood sample from the dog, processing it in a centrifuge to concentrate the platelets, and injecting the platelet-rich plasma into the affected joint.
Platelets contain numerous growth factors stored in their alpha granules including platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-β), vascular endothelial growth factor (VEGF), and insulin-like growth factor 1 (IGF-1). When platelets are concentrated and activated within an arthritic joint, the theory is that these growth factors will reduce inflammation, support tissue healing, and reduce pain.
How it's claimed to work
The proposed mechanisms include:
Anti-inflammatory effects. Platelets release factors that modulate inflammation in the joint environment.
Growth factor delivery. The various growth factors theoretically stimulate cartilage and connective tissue health.
Stem cell recruitment. PRP may help recruit and activate the body's own stem cells to the area, which is why some protocols combine PRP with stem cell therapy.
Direct analgesic effects. Some pain reduction may occur through direct mechanisms unrelated to inflammation.
Evidence, and why I'm cautious
This is where I need to be most direct.
A 2025 critical appraisal published in the Australian Veterinary Journal by Cai and Zaki reviewed seven studies of intra-articular PRP injection for canine osteoarthritis. The conclusion was direct: current evidence supporting the effectiveness of PRP in reducing pain and lameness in dogs with OA is weak, and further large randomised controlled trials are needed.
This matters, because PRP is widely marketed as effective for canine arthritis pain, and the formal evidence doesn't yet strongly support that marketing.
That said, some individual studies have shown positive effects, and clinical experience at experienced centres often reports useful outcomes in selected cases.
The realistic summary: PRP may help some dogs with arthritis, but the formal evidence base supporting its widespread use is currently weaker than the marketing implies. Owners considering PRP should do so with realistic expectations about the level of evidence supporting it.
When PRP might be reasonable to try
Despite the weak overall evidence, PRP has some characteristics that make it worth considering in specific situations:
Lower cost than stem cells. PRP is significantly less expensive than stem cell therapy, making it a lower-stakes trial of regenerative approaches.
Simpler procedure. No general anaesthesia for tissue harvest. Often performed under sedation as a single procedure.
Low risk. Adverse events from autologous PRP are rare. The treatment uses the dog's own biological material with minimal processing.
Potential combination benefits. Used alongside stem cells, PRP may enhance the overall regenerative approach.
Trial before stem cells. Some clinicians use PRP as an initial regenerative trial, moving to stem cells if PRP doesn't produce adequate response.
Realistic UK costs
PRP costs significantly less than stem cell therapy. Single intra-articular PRP injection typically costs in the region of £400-800 in UK practice, depending on the centre and how many joints are treated. Some protocols use a course of two or three injections over several weeks, which puts the total in the £800-1,500 range. Used as an add-on alongside a stem cell treatment, PRP typically adds modestly to the overall cost rather than being charged as a fully separate fee. As with all regenerative pricing, confirm directly with the centre before committing.
Hyaluronic acid injections

Hyaluronic acid is a key component of synovial fluid (the lubricating fluid in joints). It's responsible for some of the smooth, lubricated joint function we associate with healthy joints. In arthritic joints, hyaluronic acid quality and quantity is often reduced.
Intra-articular hyaluronic acid
Direct injection of hyaluronic acid into arthritic joints has been used in human medicine for some years, with mixed evidence of benefit. In veterinary practice, it's used by some centres, often as part of combined regenerative protocols.
The theoretical mechanism is improvement of joint lubrication and reduction of inflammation. The actual clinical evidence in dogs is limited.
Oral hyaluronic acid
We covered this in our supplements article. The bioavailability of oral hyaluronic acid is questionable and the evidence for its effectiveness as a supplement is weak.
Where this fits
For most dogs with arthritis, hyaluronic acid isn't a priority intervention compared to the foundational treatments and the better-evidenced regenerative options. It may have a place in combined protocols, but it's not the headline treatment.
Other emerging treatments
The regenerative medicine field is moving quickly. Several other approaches are at various stages of development and clinical introduction.
Monoclonal antibodies beyond Librela
Anti-NGF therapy (Librela for dogs, Solensia for cats) is now established. Additional monoclonal antibody treatments targeting other aspects of arthritis pain and inflammation are in research and clinical development. The specifics will evolve over the coming years.
Cell-free regenerative products
Rather than using whole cells, some approaches use the secretome (the molecules released by cells) or extracellular vesicles (exosomes) for regenerative effects. The theoretical advantages include better standardisation, easier storage, and potentially lower risk than whole-cell therapy. Clinical use in canine OA is still early.
Gene therapy
Gene therapy approaches to OA, where genes encoding therapeutic proteins are delivered directly to the joint, are in research stages. Approaches being investigated include gene therapy for sustained delivery of anti-inflammatory proteins. Not yet routinely available in clinical veterinary practice.
Allograft cartilage products
Various processed cartilage products derived from donor tissue are being developed for veterinary use. Early clinical applications include specific cartilage repair scenarios.
Growth factor injections
Beyond PRP, specific growth factor preparations (BMP-7, IGF-1, others) have been investigated for joint applications. Most remain in research stages for veterinary use.
A realistic position on all of these emerging approaches: interesting science, limited current clinical availability, evidence base still developing. The field will look quite different in five years than it does today.
Questions to ask before you say yes
If your dog has been recommended for regenerative therapy, these questions are worth asking:
What's the specific evidence base for this treatment in dogs with my dog's specific condition? Not extrapolation from human studies or other species, not laboratory studies, not testimonials. Actual clinical evidence in dogs with the relevant condition.
What's the realistic response rate? What proportion of dogs treated show meaningful improvement? When and how is that improvement assessed?
What does "improvement" actually mean? Specific measurements rather than vague claims. Pain scores? Gait analysis? Quality of life metrics? Reduction in other medications?
This is the question I'd push hardest on, because regenerative treatments cost £3,000–£9,000 and the response window stretches over months. "She seems brighter" isn't a defensible measurement for that kind of spend. Part of why we built PAWSCHECK was for exactly this situation. PAWSCHECK (pawscheck.co.uk) is a separate ConciergeVet tool that produces a vet-reviewed gait analysis from a short smartphone video, with biomechanical measurements that compare against the pre-treatment baseline, so "is the £4,000 of stem cells actually working?" becomes an answerable question rather than a feeling.
I mention this not to recommend any particular monitoring tool but to make the point that pre- and post-treatment objective measurement matters more here than in almost any other arthritis intervention. A clinic-based gait analysis, a structured pain diary, a videoed walking baseline, any of these is better than relying on impression alone. Don't agree to a several-thousand-pound treatment without agreeing in advance how you'll know whether it worked.
How long does the effect typically last? Is one treatment sufficient or are repeated treatments needed?
What's the cost over time? Including likely repeat treatments and any monitoring.
What's the success rate in this specific centre? Centres with more experience often achieve better outcomes.
What if it doesn't work? What's the next step? Will the centre refund partially if there's no response?
What's the realistic time to assess response? Weeks? Months? When will you know whether to continue or stop?
Who shouldn't have this treatment? Contraindications and situations where the centre would recommend against it.
Could I have a second opinion before proceeding? Reputable centres welcome this; pressure to commit immediately is a red flag.
What I'd recommend in practice
For owners weighing regenerative medicine for their arthritic dog, here's my candid clinical position:
Get the foundations right first. Pain medication, weight management, exercise modification, environmental adaptation, evidence-based supplements. Don't reach for expensive regenerative treatments while the basic interventions are unoptimised.
Consider hydrotherapy before regenerative medicine for most dogs. Better-evidenced, generally less expensive, often more impactful in everyday terms.
Consider acupuncture if pain control needs enhancement. Stronger evidence base than PRP for chronic pain.
Regenerative medicine has a place for specific situations: dogs failing conservative management, dogs unable to take NSAIDs, dogs whose owners specifically want to explore these options with realistic expectations.
Stem cell therapy carries more current evidence than PRP for canine OA, though both have limitations.
Set realistic expectations. These treatments may help. They're not cures. They typically work alongside other interventions, not instead of them. Response varies considerably between individual dogs.
Be a critical consumer of marketing claims. The most enthusiastic marketing often comes from centres with the most financial interest in selling the treatments. Critical evaluation matters.
Consider the cost carefully. Money spent on uncertain regenerative treatments isn't available for other interventions. For some dogs, an additional £3,000 might be better spent on optimised conventional management plus hydrotherapy than on a stem cell course of uncertain benefit.
Don't be afraid to wait. The field is evolving quickly. Treatments that aren't widely available or well-evidenced today may be considerably better characterised in two or three years.
Looking ahead
Regenerative medicine for canine arthritis is genuinely promising. The science is sound in principle, the early evidence is encouraging, and the mechanisms make sense. As the field matures, with better standardisation and more rigorous clinical trials, the picture will become clearer.
In five years, we'll likely have:
- Better evidence about which dogs benefit most
- More refined protocols (cell numbers, treatment frequencies, combination approaches)
- Lower costs as the technology becomes more accessible
- Newer approaches building on what's been learned
- Clearer guidance on when regenerative medicine belongs in the treatment algorithm
For now, the reality is that these treatments have a place, but a more limited place than the most enthusiastic marketing suggests. They're not the first thing to reach for. They're a consideration after the foundation is solid, for specific situations, with realistic expectations.
A final thought

I've been somewhat sceptical, and that deserves explanation. It isn't because I think regenerative medicine doesn't work. It's because I think owners deserve candid information when significant money is involved, and the marketing around regenerative medicine has at times outrun the evidence in ways that have damaged patient interests.
The treatments may genuinely help your dog. They may also fail to deliver the improvement you hoped for. The truthful position is uncertainty, with the responsibility to make the best decision with the available information.
If you're considering regenerative therapy for your dog, do so with eyes open. Ask the questions. Understand what the evidence does and doesn't support. Set realistic expectations. Choose a centre with genuine expertise rather than aggressive marketing. Know what you're spending and what you might get for it.
Your dog deserves the benefit of the latest treatments where they're appropriate, but they also deserve protection from being subjected to treatments whose evidence base doesn't match the cost or the hype. The sensible middle ground is where good clinical decision-making happens.
The field is moving. We'll have better answers in coming years. For now, regenerative medicine is one option in a broader toolkit, neither the panacea sometimes suggested nor the snake oil sometimes implied. Used thoughtfully, in the right cases, with realistic expectations, it has its place.
References
- Olsson DC, Teixeira BL, Jeremias TDS, Réus JC, De Luca Canto G, Porporatti AL, Trentin AG. Administration of mesenchymal stem cells from adipose tissue at the hip joint of dogs with osteoarthritis: A systematic review. Research in Veterinary Science, 2021;135:495-503.
- Brondeel C, Pauwelyn G, de Bakker E, Saunders J, Samoy Y, Spaas JH. Mesenchymal stem cell therapy in canine osteoarthritis research: "Experientia Docet" (experience will teach us). Frontiers in Veterinary Science, 2021;8:668881.
- Halperin S. Stem cells in canine osteoarthritis. Part 1: sources, effects and modes of action. Companion Animal, 2025;30(3):32-40.
- Halperin S. Stem cells in canine osteoarthritis. Part 2: case selection, choices, guidelines and outcomes. Companion Animal, 2025;30(4):2-8.
- Halperin S. Stem cells in canine osteoarthritis. Part 3: clinical evidence and practical considerations. Companion Animal, 2025;30(5):2-5.
- Cai XL, Zaki S. The effect of intra-articular platelet-rich plasma injection on pain and lameness in dogs with osteoarthritis. Australian Veterinary Journal, 2025;103(10):663-671.
- Cao M, Ou Z, Sheng R, et al. Efficacy and safety of mesenchymal stem cells in knee osteoarthritis: a systematic review and meta-analysis of randomized controlled trials. Stem Cell Research & Therapy, 2025;16(1):122.
- Sadeghirad B, et al. Mesenchymal stem cell therapy for knee osteoarthritis: a systematic review and individual participant data meta-analysis. Osteoarthritis and Cartilage, 2024;32(10):1207-1219.
Sister tool · Sightline
Track whether treatment is working
Sightline, a separate ConciergeVet tool, runs a short weekly check-in built on validated pain and mobility instruments, turns it into a single Sightline Score you can watch trend over weeks rather than judge on one bad day, and produces a report you can bring to your vet.
A written log, or our printable trackers, does much the same job.
See how Sightline tracks treatmentSee where your pet stands today
Tracking is the other half of managing arthritis. Take the 2-minute Mobility Check to see your pet's stage, then watch it shift as treatment takes effect.
Take the Mobility CheckYou're not doing this alone
Compare treatment journeys and talk to owners managing arthritis. Free to join.
Join PetsLikeMine