IVDD Surgery vs Conservative Treatment: How to Decide
Dr. Alastair Greenway
MRCVS
Surgery, or strict rest? For most owners facing intervertebral disc disease, this is the hardest call they will have to make, and it usually arrives tangled up with fear, cost, and very little time to think. The way this decision is often framed is unfair to owners. There is rarely a single "right" answer that a good owner would obviously choose, with surgery as the heroic option and rest as the cheap cop-out. That is not how this works. Two genuine paths sit in front of you, each suited to different dogs and different circumstances, and this guide gives you a fair, structured way to weigh them: by grade, by deep pain, by time, by what you can realistically manage, and by what your vet advises. I am not going to push you toward surgery, and I am not going to shame you for choosing rest. I am going to give you the real figures and help you decide well.
Two real paths, not a right and a wrong one
Start with this: the best choice genuinely depends on a handful of specific factors, and it changes from dog to dog. It depends on the grade, how severely the spinal cord is affected. It depends on whether deep pain is present, the single biggest factor in the outlook. It depends on how much time has elapsed since the signs began. It depends on whether you can get to an MRI scanner and a surgeon quickly. It depends, frankly, on what you can afford. And it depends on the individual dog and your own circumstances, your home, your time, your ability to nurse a recovering dog for weeks.
No article, and no website, can make this decision for you, because it is not a single medical fact, it is a weighing of all of those things together for your particular dog. What this guide can do is lay out the two paths clearly, give you the recovery and recurrence figures for each so you are deciding on evidence rather than fear, and provide a framework to work through with your vet. This is a decision you and your vet make together, and it deserves to be made with real information.
Conservative management: what it is and who it suits
Conservative, or medical, management means treating the disc problem without surgery, and it rests on two pillars: strict rest and pain relief. Rest is the heart of it, typically four to six weeks of genuinely strict confinement, which our dedicated guide to crate rest covers in full, because done properly it is far more demanding than "taking it easy." You are giving the injured disc and the inflamed spinal cord time and stability to settle, and the body time to lay down stable scar tissue, undisturbed by movement. Interestingly, studies show recovery on this path is not actually dependent on the compression resolving. The cord can recover function even while some compression remains, which is part of why rest works at all.
Alongside the rest comes pain relief, and modern practice here is specific and worth getting right. Today's approach is built around a non-steroidal anti-inflammatory drug, an NSAID, usually combined with gabapentin and sometimes a muscle relaxant called methocarbamol, which our medications guide explains in detail. Crucially, steroids are not part of this picture, and we will come to the strong evidence behind that below, but the short version is that an NSAID and a steroid must never be given together, and human painkillers must never be given at all.
Who does conservative management suit? It is most appropriate for the milder grades, and the success rates are genuinely good for them. For dogs in pain but still walking, or wobbly but still on their feet, the grade 1 and grade 2 dogs, around ninety percent recover with rest and medication, and some studies of the mildest cases report virtually all recovering. It can also suit selected grade 3 dogs, those that cannot walk but retain some leg movement, in discussion with your vet, though here surgery begins to offer an advantage. It is only fair, though, to be clear about two real limits. One is that success falls as severity rises: a grade 3 dog managed medically recovers perhaps seventy percent of the time against around ninety percent with surgery, and a paralysed grade 4 dog only about fifty percent of the time medically. The other is recurrence: another episode at some point is common after conservative management, reported in anywhere from fifteen to sixty-six percent of dogs depending on the dog and the study, and indeed around half of ambulatory dogs treated with rest and anti-inflammatories in one series went on to relapse. And conservative management can fail outright: if a dog on strict rest deteriorates, becoming weaker or losing the ability to walk, or if the pain cannot be controlled despite proper treatment, that is the signal that the situation has changed and surgery should be reconsidered, promptly. Conservative management is not "do nothing and hope"; it is an active treatment that needs monitoring, with a clear plan for switching course if the dog goes the wrong way.
Surgery: what it is and who it suits
Surgery for IVDD aims to physically remove the herniated disc material that is pressing on the spinal cord, relieving the compression directly. It usually begins with an MRI scan to pinpoint exactly which disc is the problem and where, because the surgeon needs to know precisely where to operate. The operation itself is typically a procedure called a hemilaminectomy for disc disease in the back, or a ventral slot for disc disease in the neck, in which a small window is made in the bone to reach and remove the offending disc material. Some surgeons also fenestrate adjacent discs during the same operation, removing their inner material to try to prevent a future extrusion there, though the evidence on whether this reduces recurrence is mixed and it is a judgement your surgeon will make.
Who does surgery suit? It is typically advised for the more severe grades, the dogs that can no longer walk, grades 3, 4, and 5, and especially where deep pain status raises the stakes, and the prognosis figures are where its advantage becomes clear. For a paralysed dog that still has deep pain present, a grade 4 dog, surgery offers an excellent outlook, with recovery reported in around eighty to ninety percent of cases against roughly fifty percent with medicine alone. Studies of non-ambulatory but deep-pain-positive dogs treated surgically have found very high recovery, in the region of eighty-six to ninety-six percent walking again, typically within about two weeks. For a dog that has lost deep pain, a grade 5 dog, the picture is more serious but far from hopeless: surgery offers a recovery rate averaging around sixty percent, against under five percent with medicine alone, and this is the situation where time matters most. Recovery from surgery is not instant, it involves a hospital stay of a few days followed by weeks of restricted activity and rehabilitation at home, much like the conservative route in its demands on you. And surgery is not immune from recurrence either, with another disc going at some point reported in roughly three to over forty percent of surgically treated dogs, though for most dogs this is lower than after conservative management alone. But for the right dog, particularly a severely affected one, surgery offers the best chance of getting back on its feet.
Deep pain and time: the two threads that matter most
Two threads run through everything above and deserve drawing out on their own, because they are what make some of these decisions urgent rather than considered. First, deep pain, and it needs stating precisely. Deep pain perception is a conscious response to a firm toe-pinch, the dog turning, crying, or looking round, not the reflex twitch of a leg pulling back on its own, which can happen with no sensation reaching the brain at all. Its presence or absence is the biggest single predictor of recovery, which is why your vet assesses it so carefully and why it weighs so heavily in the surgery decision.
Then time, specifically for the dog that has lost deep pain. For these grade 5 dogs the odds are genuinely time-sensitive: operating within around forty-eight hours of the signs starting has carried roughly a sixty percent chance of recovery, whereas leaving it toward a week or more has seen that fall steeply, in some reports to under ten percent. So this is the scenario where "let us wait and see" can be the wrong call, because delay can erode the chance. I want to be precise, though, and avoid a myth that frightens owners unnecessarily: this does not mean there is a rigid cut-off of a day or two after which surgery is pointless. Dogs that had lost deep pain for a week or more before surgery have still gone on to recover in the published literature, so the door does not slam shut at forty-eight hours. The real message is therefore urgency, not panic: for a severely affected dog, especially one without deep pain, make the decision quickly rather than sitting on it, because the surgical window, while not a hard door, does narrow with time.
A decision framework you can actually use
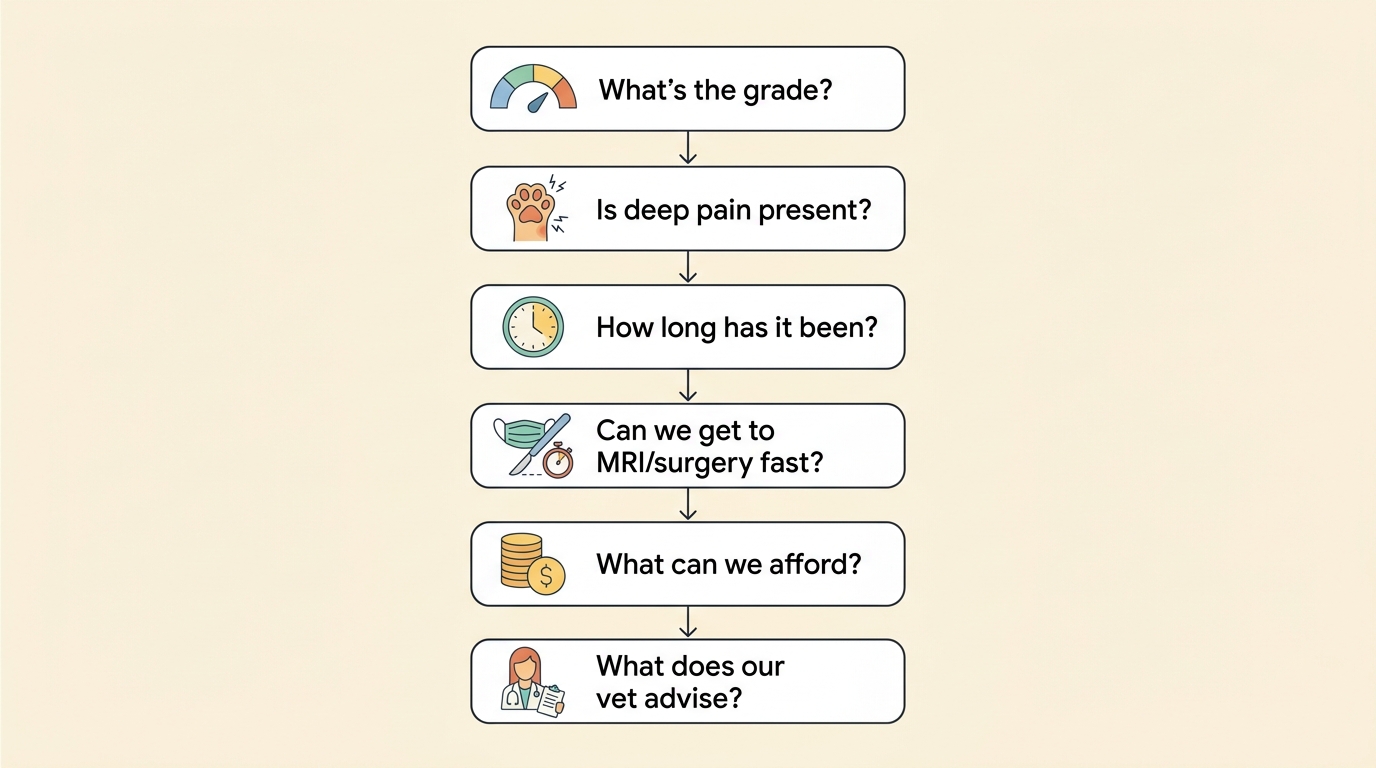
Rather than leave you with "it depends," here is a set of questions you can work through, with your vet, that will steer you toward the path that fits your dog. Each one nudges the decision.
First, what is the grade? Milder grades, dogs still walking, lean toward conservative management, where the odds are good; more severe grades, dogs that cannot walk, lean toward surgery, where the advantage over rest widens with severity. Second, is deep pain present? Its presence is reassuring and widens your options; its absence makes surgery more urgent and the situation more serious. Third, how long has it been? A recent, sudden, severe loss of function points toward acting fast; this is not a decision to deliberate over for days in a severely affected dog. Fourth, can you access MRI and surgery quickly? Surgery is only an option if you can reach a referral centre with a scanner and a surgeon in a useful timeframe, so practical access is part of the real-world decision. Fifth, what can you realistically afford? This is a legitimate question, not a shameful one, and we will come to it squarely in a moment. And sixth, what does your vet advise? Your own vet, and where appropriate a neurologist, knows your individual dog and is your most important guide. Working through these questions turns a frightening fog into a structured choice, and our IVDD decision worksheet is built to help you do exactly that, on paper, calmly.
What about steroids?
It is worth pausing on steroids specifically, because older advice, and even some lingering habits, may have you expecting them, and the evidence here is now clear enough to settle the question. For years, high-dose steroids were given for acute spinal cord injury on the logic that they reduce inflammation. But when this was finally put to a proper test, a placebo-controlled, randomised, blinded trial in dogs paralysed and deep-pain-negative from disc herniation, high-dose methylprednisolone showed no benefit over a dummy treatment. There is, at present, no proven medical drug that counters the secondary damage to the spinal cord, which is precisely why prompt, appropriate treatment and, where indicated, surgery matter more than any injection.
Worse, steroids in this setting carry real harm. Dachshunds given high-dose steroids around spinal surgery suffered significantly more gastrointestinal complications and needed more gut-protective medication, and high doses of certain steroids in dogs with acute spinal injury have been linked to fatal perforation of the bowel. That is why the modern approach has moved firmly to the NSAID-led pain relief described above, and why there is one absolute rule worth carrying away: steroids and NSAIDs must never be given together, as the combination sharply raises the risk of serious gut ulceration and bleeding. If you have ever wondered why your vet did not put your paralysed dog on steroids, this is the answer, and it reflects good, up-to-date medicine, not a gap in care.
Money, plainly
It would be wrong to discuss this decision without talking about money, because for many families it is one of the real factors, and pretending otherwise helps no one. So let me be plain, with figures, while noting these are typical UK ranges that vary by region and centre and are best confirmed with your own practice. Surgery, with its MRI, the operation, and the hospital stay, is a major expense, commonly running to somewhere around six to ten thousand pounds, with the MRI alone often two to three thousand, though some referral centres offer lower fixed-price packages for straightforward cases, particularly in small dogs, in the region of four to four and a half thousand. Conservative management is far cheaper, but it is not free, it still involves veterinary consultations, weeks of medication, very possibly a proper pen and some physiotherapy, and a great deal of your own time and energy over those weeks. Our dedicated guide to what IVDD costs in the UK lays all of this out in detail.
The single most important money point is insurance: if your dog is insured under a suitable lifetime policy taken out before any signs appeared, much of the cost of surgery may be covered, which can change the decision entirely, whereas the absence of cover, or a policy with low limits, is a real constraint that it is entirely reasonable to factor in. There is no shame in cost being part of this decision. A loving owner who cannot find many thousands of pounds for surgery, and who therefore pursues good conservative management, is making a responsible, caring choice, not failing their dog, especially given that for the milder grades the recovery odds with rest are genuinely good. Money is a legitimate part of weighing this up, and a good vet will discuss it openly with you, including whether fixed-price options or payment arrangements might help.
The emotional part
Finally, the part that the clinical discussion often leaves out: this decision is emotionally hard, and whatever you choose, you may second-guess it. That is normal, and it is worth addressing head on. Owners who choose surgery sometimes feel guilt if recovery is incomplete; owners who choose conservative management sometimes worry they did not "do everything"; and owners who, for cost or for the dog's sake, decline surgery altogether can carry a particularly heavy guilt. I want to lift some of that weight: choosing conservative management is a legitimate, evidence-backed treatment with good odds in the milder grades, not a failure to act, and there are even circumstances, with certain dogs and certain severities, where declining surgery and focusing on comfort, or making harder decisions still, can be the kindest and most loving choice of all. Our more sensitive guides, on quality of life and on the hardest decisions, are there for those moments, gently, if you need them.
What matters is that you make the decision thoughtfully, with good information and your vet's guidance, in your dog's genuine best interests and within your real circumstances. So take the questions above, work through them on our decision worksheet, bring the neurologist questions checklist to your appointment if surgery is on the table, and talk it through properly with your vet or a neurologist.
References
- Olby NJ, Moore SA, Brisson B, Fenn J, Flegel T, Kortz G, Lewis M, Tipold A. ACVIM consensus statement on diagnosis and management of acute canine thoracolumbar intervertebral disc extrusion. Journal of Veterinary Internal Medicine, 2022;36(5):1570-1596.
- Jeffery ND, Barker AK, Hu HZ, Alcott CJ, Kraus KH, Scanlin EM, Granger N, Levine JM. Factors associated with recovery from paraplegia in dogs with loss of pain perception in the pelvic limbs following intervertebral disk herniation. Journal of the American Veterinary Medical Association, 2016;248(4):386-394.
- Pancotto T. Saved from the sidelines: conservative management of intervertebral disk disease. dvm360, 2013.
- Pancotto T. Making the cut: surgical versus medical management of canine disk disease. dvm360, 2013.
- Ferreira AJ, Correia JH, Jaggy A. Thoracolumbar disc disease in 71 paraplegic dogs: influence of rate of onset and duration of clinical signs on treatment results. Journal of Small Animal Practice, 2002;43(4):158-163.
- Olby NJ, Muguet-Chanoit AC, Lim J-H, et al. A placebo-controlled, prospective, randomized clinical trial of polyethylene glycol and methylprednisolone sodium succinate in dogs with intervertebral disk herniation. Journal of Veterinary Internal Medicine, 2016;30(1):206-214.
- Boag AK, Otto CM, Drobatz KJ. Complications of methylprednisolone sodium succinate therapy in Dachshunds with surgically treated intervertebral disc disease. Journal of Veterinary Emergency and Critical Care, 2001;11(2):105-110.
- Toombs JP, Collins LG, Graves GM, Crowe DT, Caywood DD. Colonic perforation in corticosteroid-treated dogs. Journal of the American Veterinary Medical Association, 1986;188(2):145-150.
- Mann FA, Wagner-Mann CC, Dunphy ED, et al. Recurrence rate of presumed thoracolumbar intervertebral disc disease in ambulatory dogs with spinal hyperpathia treated with anti-inflammatory drugs: 78 cases (1997-2000). Journal of Veterinary Emergency and Critical Care, 2007;17(1):53-60.
- Dachshund IVDD UK. Insurance and the cost of IVDD treatment.
Free downloads
Companion worksheets to put what you've read into practice. Free PDFs, print at home.

Surgery vs Conservative: Decision Worksheet
PDF · 284 KBA calm way to weigh the hardest choice in IVDD while the clock is ticking. Grade, deep pain, time since the signs began, cost and your own circumstances, laid out side by side so the decision is structured rather than panicked. Take it into the consult and fill it in together with your vet.

Neurologist Questions Checklist
PDF · 204 KBWalking into a referral appointment is easier with the right questions already written down. What the MRI showed, what each option really offers your dog, the honest odds, the aftercare and the cost, grouped so you leave understanding the plan. Tick the ones that matter to you and add your own.
Sister tool · Sightline
Track whether treatment is working
Sightline, a separate ConciergeVet tool, runs a short weekly check-in built on validated pain and mobility instruments, turns it into a single Sightline Score you can watch trend over weeks rather than judge on one bad day, and produces a report you can bring to your vet.
A written log, or our printable trackers, does much the same job.
See how Sightline tracks treatmentTrack the recovery, day by day
Recovery from a disc injury is all about the trend. Log the daily milestones through crate rest and rehab so you can see real progress, not just good and bad days.
Open the Recovery TrackerYou're not doing this alone
Compare treatment journeys and talk to owners managing IVDD. Free to join.
Join PetsLikeMine