Central Sensitisation: When Pain Becomes Its Own Disease
Dr. Alastair Greenway
MRCVS, 25 years clinical experience
Modern pain medicine has a concept that explains a great deal of what we see in chronic pain patients, yet owners rarely hear it named. It's called central sensitisation, and once you understand it, the way you think about your dog's arthritis shifts.
I've touched on it in passing across several other articles in this space, but the implications run deep. Central sensitisation explains why some dogs don't respond well to standard pain medications. It explains why catching arthritis early matters so much, and why multimodal pain management is now considered the standard of care. It explains why dogs whose pain has been managed inadequately for years sometimes need far more intensive treatment than dogs whose pain was caught early. And it explains why the relationship between joint damage on an X-ray and the amount of pain a dog feels is so unreliable.
If any of those things have confused you, understanding central sensitisation should help. If you've been frustrated that your dog's treatment isn't working as well as you'd hoped, it may explain why. And if your dog's arthritis was caught early and is being managed well, it'll help you see why that's such a valuable position to be in.
What pain actually is
Most people picture pain as a direct experience: tissue damage produces pain signals, the signals travel to the brain, and the brain creates the experience of hurting. The amount of damage equals the amount of pain. Simple cause and effect.
The reality is far more complex.
Pain is a constructed experience. It's the result of complex processing in the nervous system that integrates signals from peripheral tissues with input from the spinal cord, the brain, past experience, current attention, expectation, mood, and many other factors. The same tissue injury can produce very different amounts of pain in different individuals, or even in the same individual at different times.
This holds true in humans, and it holds true in dogs. A dog's experience of pain isn't just a direct readout of joint damage. It's the result of how the nervous system is processing and amplifying the signals coming from the damaged joints. And that processing can change over time.
Why does this matter? Because it means pain isn't fixed. It can be modulated. The nervous system can be turned up or turned down. And in chronic pain conditions, the system frequently gets turned up over time, in ways that carry profound implications for how the disease is experienced and how it should be treated.
How the pain system works when all is well
In a healthy nervous system, pain signals work roughly like this.
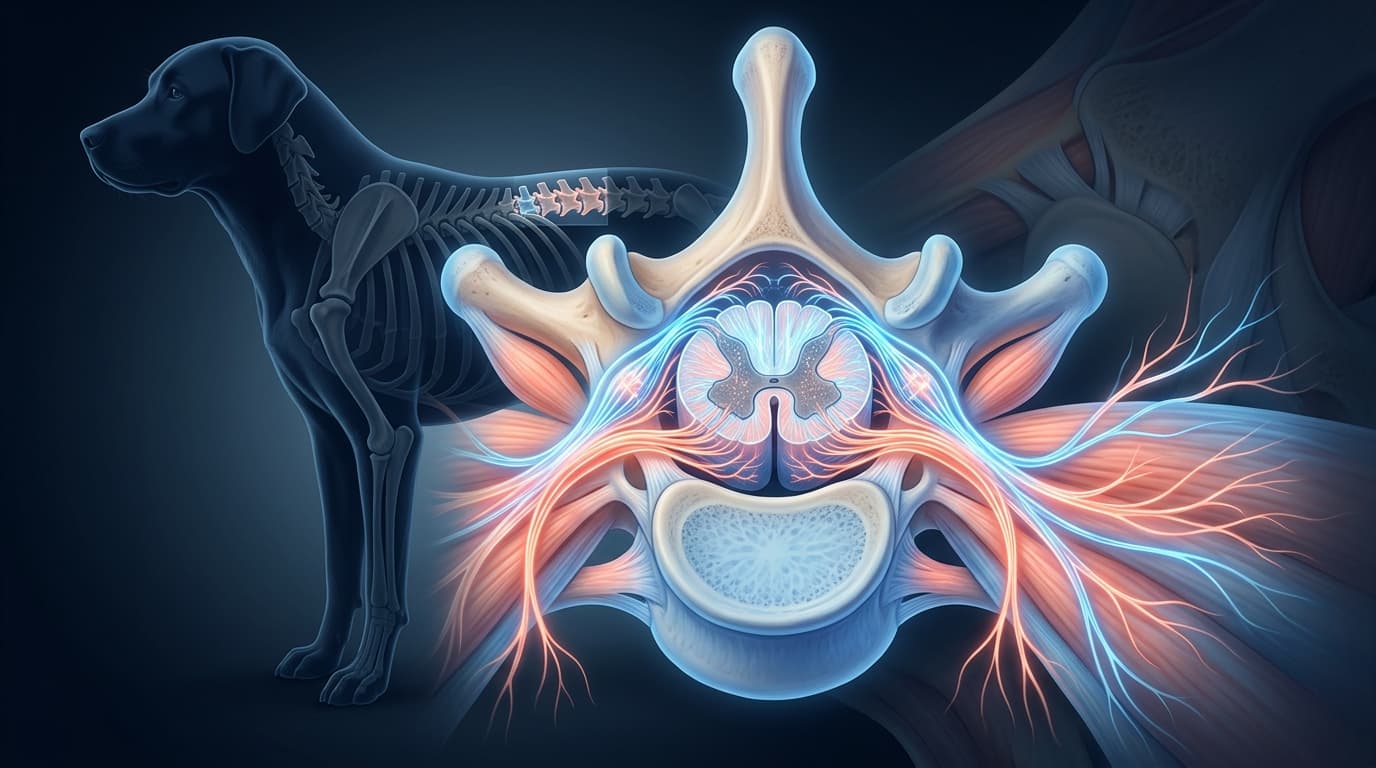
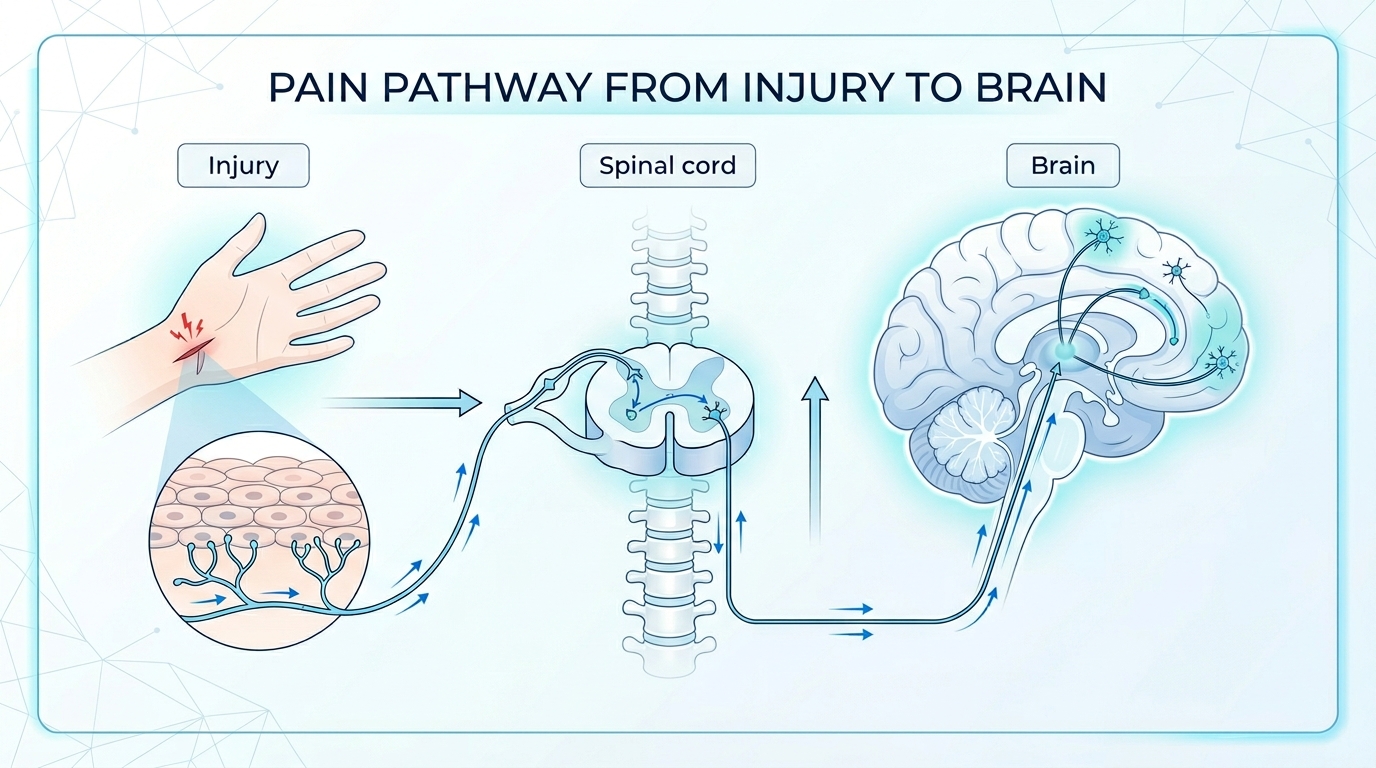
Specialised nerve endings called nociceptors are scattered throughout the body. When tissue is damaged or threatened (by heat, cold, pressure, chemicals, or inflammation), these nociceptors fire and send electrical signals along nerve fibres toward the spinal cord.
In the spinal cord, those signals pass through "switchboards" called the dorsal horns, where they're processed and modulated. Some signals are amplified, others are suppressed. Inhibitory signals from the brain travel down to the spinal cord to "turn down" pain signals when appropriate. Excitatory signals can amplify pain signals when the brain decides they need more attention.
The processed signals then travel up to the brain, where they're integrated with countless other inputs to produce the conscious experience of pain.
Normally this whole system is well calibrated. Mild injuries produce mild pain. Significant injuries produce significant pain. The pain settles as the injury heals. The system returns to baseline.
In chronic pain, this elegant calibration starts to break down.
How chronic pain rewires the system
When pain signals keep arriving at the spinal cord and brain over weeks, months, and years, the nervous system itself begins to change. This isn't a metaphor. It's actual physical and chemical change in nerve cells, their connections, and their behaviour.
These changes happen at multiple levels.
At the site of damage (peripheral sensitisation), the nociceptors themselves become more responsive. They start firing at lower thresholds. They multiply in number. Inflammatory chemicals released around the damaged tissues sensitise these nerve endings further. The result is that the same level of tissue damage produces more pain signals than it would have done initially.
In the spinal cord (central sensitisation), the dorsal horn neurons that receive pain signals become hyper-responsive. The thresholds for firing drop. The amplification increases. The descending inhibitory pathways from the brain become less effective at turning down the signals. The spinal cord becomes increasingly efficient at transmitting and amplifying pain signals.
In the brain, attention to pain signals increases. Pain processing areas may expand. Emotional responses to pain change. The brain becomes more responsive to pain inputs and may even generate pain signals from much smaller peripheral inputs than would normally trigger them.
Taken together, these changes mean the pain system becomes increasingly sensitive over time. Stimuli that wouldn't normally hurt start to. Painful stimuli become more painful. The relationship between actual tissue damage and pain experience becomes increasingly disconnected.
In the most advanced cases, pain can be generated by the nervous system itself, with little or no peripheral input required. The pain has become its own condition, separate from the original cause.
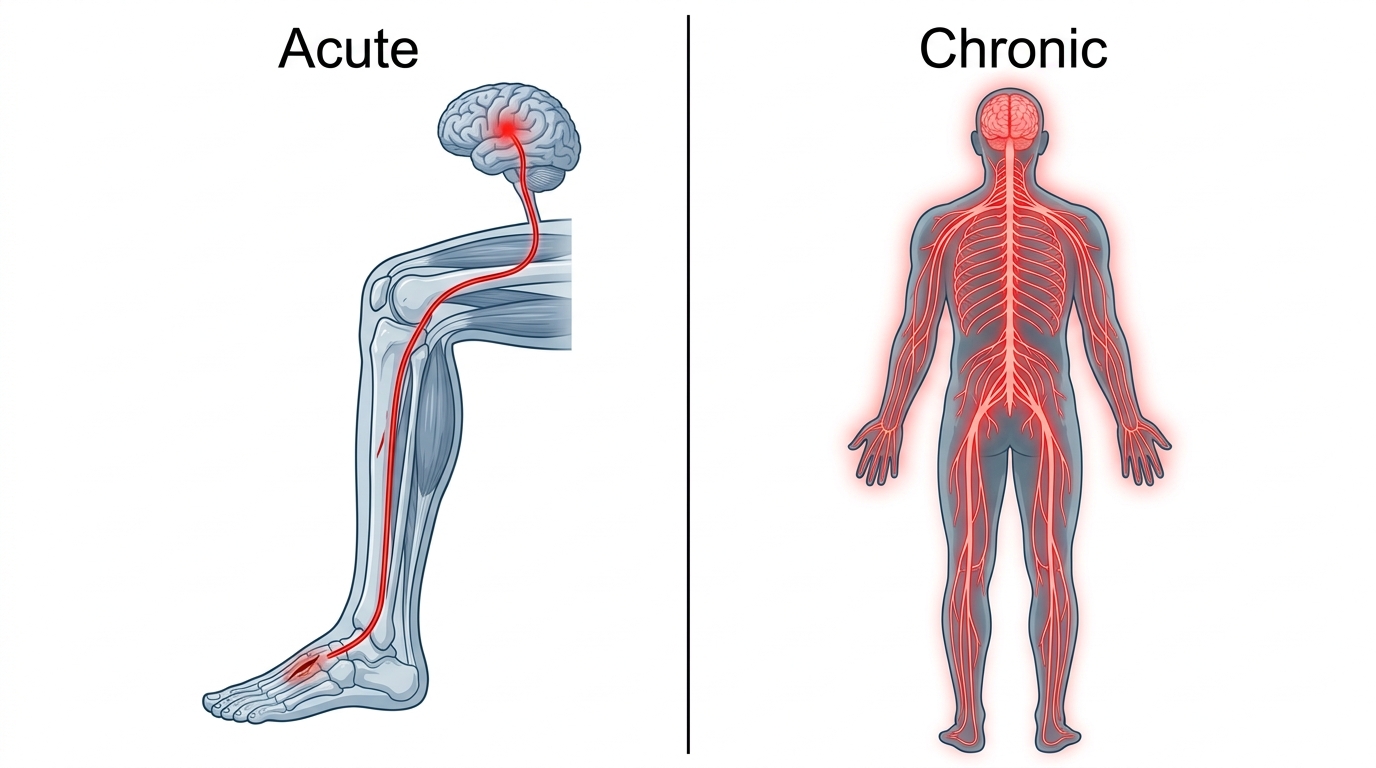
This is central sensitisation. And it's the single most important concept in understanding why chronic pain is so different from acute pain, and so much harder to treat.
What this looks like in dogs
The evidence that central sensitisation occurs in dogs with osteoarthritis is now substantial. Research using techniques borrowed from human pain medicine, including quantitative sensory testing, has demonstrated that dogs with chronic arthritis show measurable signs of central sensitisation.
A 2018 UK study by Hunt and colleagues, using electrophysiological measurements in dogs with naturally occurring osteoarthritis, demonstrated reduced efficacy of the descending pain inhibition pathways. In other words, the systems that should be turning down pain signals were working less effectively in these dogs.
Studies in cats point in a similar direction. A 2017 study led by Monteiro, using a technique called response to mechanical temporal summation, found a facilitated temporal-summation pattern in cats with osteoarthritis: a sign that the nervous system was amplifying repeated pain inputs rather than dampening them. A 2020 meta-analysis by the same group, looking across multiple feline studies, confirmed the finding.
What does this look like clinically? The classic signs of central sensitisation in chronic arthritis include:
Pain that's disproportionate to the visible joint changes. A dog with relatively modest X-ray findings but clear signs of significant pain may have central sensitisation amplifying the input from the joint.
Pain in areas distant from the original problem. Dogs with hip arthritis who develop sensitivity in their backs or front legs may be showing widespread sensitisation that's spread beyond the original area.
Reluctance to be touched or handled in areas that have no obvious local pathology. The "grumpy old dog" who doesn't want to be petted may have central sensitisation making normal touch feel uncomfortable.
Behavioural changes including anxiety and reactivity that go beyond what would be expected from the joint disease alone. Chronic pain affects mood and behaviour in ways that aren't always proportional to the apparent physical disease.
Poor response to standard pain medications. Dogs whose pain doesn't respond well to NSAIDs may have central components that NSAIDs don't address effectively.
Pain flares triggered by minor events. A small injury, a colder day, a slightly longer walk, that wouldn't normally cause significant pain produces a disproportionate flare-up.
Difficulty being settled or comfortable in ways that don't fit any specific positional or activity pattern. The dog seems generally uncomfortable rather than specifically painful in one location.
If any of this sounds like your dog, central sensitisation may be part of what's happening.
Why this matters for treatment
Once you understand central sensitisation, several aspects of arthritis treatment make more sense.
Why multimodal pain management is now standard
The traditional approach to pain management was to treat the local source of the pain. Inflamed joint? Anti-inflammatory drug. Job done.
We understand it differently now. For chronic pain, you need to treat the system as well as the source. A drug that reduces joint inflammation doesn't necessarily address the central sensitisation that has developed in response to that inflammation. A different drug, working through a different mechanism, may be needed alongside.
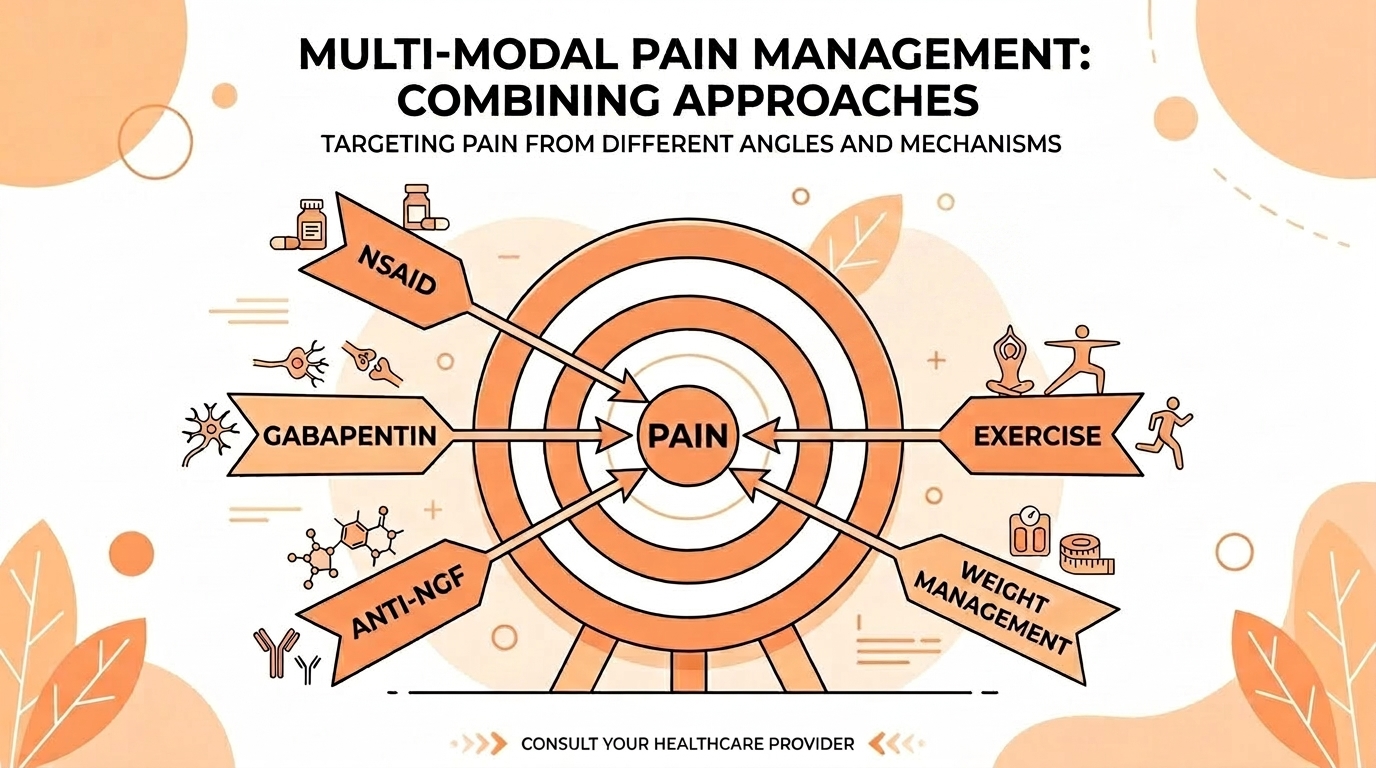
That's why a dog with longstanding arthritis often does best on a combination of medications. The NSAID addresses the joint inflammation. Gabapentin or amantadine may address the central sensitisation. Anti-NGF therapy (Librela) addresses the nerve growth factor-driven sensitisation specifically. Each mechanism contributes a different piece of the pain control puzzle, and the combination often works better than any individual drug at higher dose.
Why early treatment matters so much
If the nervous system is gradually getting "wound up" by chronic pain signals, then the longer the pain goes untreated, the more sensitisation develops, the harder it becomes to treat, and the more complex the management needed.
That's why we've become more proactive about pain control in arthritis. The old approach of "let's wait and see if she gets worse" before starting treatment has fallen out of favour. As things stand, early, effective pain control may prevent or reduce the development of central sensitisation, leading to better long-term outcomes.
A young dog whose arthritis is diagnosed at age two and well managed throughout their life may avoid the development of significant central sensitisation. An older dog whose arthritis has been progressing untreated for years almost certainly has some degree of central sensitisation that needs to be addressed.
Why X-ray findings don't predict pain
Here's one of the most clinically confusing aspects of arthritis, and central sensitisation explains it.
X-rays show structural damage to the joint. They show osteophytes, joint space narrowing, subchondral sclerosis, soft tissue swelling. What they don't show is anything about the nervous system.
A dog with dramatic X-ray findings may have a nervous system that's still functioning well, with effective descending inhibition turning down the pain signals. They cope well, function relatively normally, and don't need much medication.
A dog with much milder X-ray findings may have significant central sensitisation amplifying every signal from the joint, plus generating pain that has little to do with the original joint damage. They function poorly and need significant medical management.
An X-ray tells you about the structure. It doesn't tell you about the experience. That's why two dogs with seemingly similar disease can require very different treatment.
Why some dogs need adjunct medications
When an arthritic dog isn't responding well to NSAIDs alone, the typical pattern is to add a different class of drug rather than just increasing the NSAID dose. Central sensitisation is the reason. NSAIDs work primarily on peripheral inflammation. They don't directly address central nervous system changes.
Drugs like gabapentin work on calcium channels in nerve cells, dampening the hyperactive signalling in sensitised nerves. Amantadine works on NMDA receptors in the brain and spinal cord, addressing the wind-up phenomenon. These adjunct medications target central sensitisation directly.
That's why a dog whose pain isn't well controlled on an NSAID often improves dramatically when gabapentin or amantadine is added. We're not just adding more painkiller. We're targeting a different mechanism of pain.
Why pain management is a long-term commitment
Once central sensitisation has developed, it doesn't necessarily go away just because the original pain is treated. The nervous system has rewired itself. Reversing those changes takes time, sustained pain control, and consistency.
This is one reason arthritis treatment is rarely a "course" of medication. It's a long-term commitment to keeping the pain system as quiet as possible, so the sensitisation can gradually settle and so further sensitisation is prevented.
Dogs who do well on their pain management for months or years, then have the medication stopped because they "seem fine", sometimes show dramatic deterioration. The pain that returns isn't just from the joint damage that was always there. It's from the central sensitisation that was being suppressed by the medication and which now flares back up.
What you can do
Understanding central sensitisation gives you a framework for thinking about your dog's pain management. Several practical implications follow.
Take pain seriously from early on. Don't accept "she's just slowing down with age" as a reason to delay treatment. The longer the pain runs unmanaged, the more central sensitisation can develop. Push for proper assessment and proper treatment.
Don't accept inadequate pain control. If your dog is on medication but still seems uncomfortable, that's not "as good as it gets." Talk to your vet about adjusting, adding adjunct medications, or considering specialist referral. There's almost always something more that can be done.
The practical problem is that "still seems uncomfortable" is harder to judge than it sounds. When you see your dog every day, gradual under-control looks like normal life. That's one of the reasons we built Sightline. Sightline (sightline.vet) is a separate ConciergeVet tool that scores pain and quality of life weekly and plots the trajectory, which makes "is the current plan still good enough?" an answerable question rather than a feeling.
I mention this because the central sensitisation argument only matters if you can actually tell whether your dog is winding up or settling. A short written log does it. A monthly photograph and video does it. A structured tool does it. The point is to have some external check on your own perception, because chronic pain is exactly the sort of thing the daily eye learns to stop seeing.
Be consistent with treatment. Stopping and starting medication is one of the worst things you can do for central sensitisation. Each time the pain breaks through, the system gets wound up again. Consistent control matters.
Don't dismiss behavioural changes. A grumpy dog, a reactive dog, a dog who's "not themselves" may be telling you that pain is poorly controlled or that sensitisation is increasing. These signs are worth taking to your vet.
Address pain flares promptly. If your dog has a worse day or week, don't just wait it out. Each pain flare is potentially feeding the sensitisation system. Reach out to your vet about temporary medication adjustments or interventions to break the flare quickly.
Consider all the components of pain. Joint disease is one input. Anxiety, sleep quality, weight, exercise patterns, environment, all influence the pain experience. Optimising all of these makes the pain system easier to manage.
Don't fear medication. Some owners worry about "starting them on tablets" or about long-term medication use. The alternative, inadequately treated chronic pain leading to severe central sensitisation, is far worse. Appropriate medication, used consistently, is genuinely protective of your dog's long-term comfort.
Can it be reversed?
A reasonable question is whether central sensitisation is reversible. The answer is: partly.
Some degree of central sensitisation can be reduced with sustained good pain control. The nervous system has some capacity to "calm down" when the chronic inputs are reduced. Dogs whose pain is well controlled for months may gradually become less sensitised over time.
Complete reversal, though, is uncertain. Some of the changes (particularly in synaptic connections and neuroplasticity) may be permanent or only slowly reversible. The longer and more severe the sensitisation, the more entrenched it becomes.
This is why prevention is so much more powerful than treatment. A dog whose nervous system never develops significant sensitisation is in a fundamentally better position than one who needs to recover from years of unmanaged chronic pain.
A note about other chronic pain conditions
This article focuses on osteoarthritis, because that's the most common chronic pain condition in dogs, but central sensitisation applies to other chronic pain states as well.
Dogs with chronic back pain, cruciate disease, IVDD, or other persistent musculoskeletal problems develop similar patterns. Dogs with chronic dermatological conditions can develop neuropathic and central pain components. Dogs with cancer pain often have central sensitisation contributing to their experience.
The principles of multimodal management, early intervention, and consistent treatment apply across all these conditions.
The broader implications
There's a wider point worth making here.
In the past, chronic pain was often dismissed as "just" pain. Not life-threatening. Not visible on X-ray. Not as urgent as other diseases. The development of pain medicine as a discipline, in both human and veterinary contexts, has changed that view.
Chronic pain is now recognised as a disease state in its own right. The changes in the nervous system are real, measurable, and physiologically significant. They affect not just pain experience but mood, behaviour, sleep, immune function, and general wellbeing.
Treating chronic pain effectively isn't just about making your dog more comfortable, although that would be reason enough. It's about preventing the cascading consequences of an unwell pain system. It's about preserving brain function and behavioural integrity. It's about supporting overall health.
This is why I get a bit evangelical about good pain management for arthritic dogs. The stakes are higher than they appear.
A final thought

The takeaway isn't that arthritis is more frightening than you thought. It's that pain matters more than you might have realised, that early and consistent treatment is more valuable than you might have guessed, and that the choices you make about your dog's pain management have implications that extend beyond simple comfort.
Your dog has a nervous system that's been adapting to whatever pain experience they've had. With good management, that adaptation can be minimised, the sensitisation contained, the long-term picture improved. The relationship between your dog's joint disease and their pain experience isn't fixed. It's something you can influence.
That's genuinely empowering. The work you do, the medications you give consistently, the conversations you have with your vet, all of it contributes to a nervous system that's calmer and a dog who's more comfortable. Day by day, month by month, year by year, it adds up.
Your dog isn't just managing arthritis. They're being protected from the cumulative effects of chronic pain on the entire nervous system. That's worth doing well.
References
- Hunt JR, Goff M, Jenkins H, et al. Electrophysiological characterisation of central sensitisation in canine spontaneous osteoarthritis. Pain, 2018;159(11):2318-2330.
- Monteiro BP, Klinck MP, Moreau M, Guillot M, et al. Analgesic efficacy of tramadol in cats with naturally occurring osteoarthritis. PLoS One, 2017;12(4):e0175565.
- Monteiro BP, Otis C, Del Castillo JRE, et al. Quantitative sensory testing in feline osteoarthritic pain: a systematic review and meta-analysis. Osteoarthritis and Cartilage, 2020;28(7):885-896.
Sister tool · Sightline
Track whether treatment is working
Sightline, a separate ConciergeVet tool, runs a short weekly check-in built on validated pain and mobility instruments, turns it into a single Sightline Score you can watch trend over weeks rather than judge on one bad day, and produces a report you can bring to your vet.
A written log, or our printable trackers, does much the same job.
See how Sightline tracks treatmentSee where your pet stands today
Tracking is the other half of managing arthritis. Take the 2-minute Mobility Check to see your pet's stage, then watch it shift as treatment takes effect.
Take the Mobility CheckYou're not doing this alone
Compare treatment journeys and talk to owners managing arthritis. Free to join.
Join PetsLikeMine