Hepatic Encephalopathy: The Staring, Circling and Seizures
Dr. Alastair Greenway
MRCVS
Your dog stops mid-room and stares at nothing. He presses his head into the corner and stands there. He circles, or paces, or seems suddenly not to know where he is, or walks into furniture as though he cannot see. Maybe it happens most after dinner. Maybe someone has said the word "epilepsy" and it has lodged in your mind. You are watching your dog behave like a stranger, and you want to know what is happening and whether it is dangerous.
Here is the short version, and it matters: if your dog has a liver problem, especially a shunt, these signs may not be epilepsy at all. They may be hepatic encephalopathy, which is the brain being affected by toxins the liver should have cleared. It looks a lot like epilepsy, it is often mistaken for it, and the treatment is different. It can also become an emergency very quickly. This piece explains what to look for, why it happens, how it differs from epilepsy, and what to do.
What hepatic encephalopathy actually is
The liver is the body's filter. Blood coming from the gut carries waste products, and ammonia is the important one here, and a healthy liver processes them before they reach the rest of the body. When the liver cannot do that job, whether because blood is bypassing it through a shunt or because the liver itself is failing, those toxins build up in the bloodstream and reach the brain. The brain does not cope well with them, and the result is a collection of neurological signs that come and go: this is hepatic encephalopathy, often shortened to HE.
The key word is that it comes and goes. Because it is driven by the level of toxins in the blood, HE tends to wax and wane, and it is classically worse after a protein-rich meal. Protein is broken down into, among other things, ammonia, so a big meaty meal can tip a borderline dog over the edge a few hours later. That post-meal pattern is one of the most useful clues you can give your vet.
HE turns up most often in two groups of dogs: young dogs with a congenital liver shunt (see the piece on shunts and the surgery-versus-medical decision), and older dogs whose liver is failing, sometimes with acquired shunts. Cats can develop hepatic encephalopathy too, most often alongside significant liver disease, and the same principle applies: the signs are the brain reacting to toxins the liver should have cleared. The signs described below are written with dogs in mind, because that is where owners meet HE most often, but the underlying story is the same in a cat.
The severity of HE is not fixed; it moves up and down a scale. At the mild end a dog might just seem a little dull or subtly off. Further along come the classic signs, the staring, circling and disorientation. At the severe end a dog can become stuporous, seizure, or slip towards a coma-like state. Knowing that it is a spectrum matters, because it means a dog who is "a bit vacant" today can, if things are not addressed, be much worse another day, and it is why the mild signs are worth taking seriously rather than shrugging off.
What it looks like
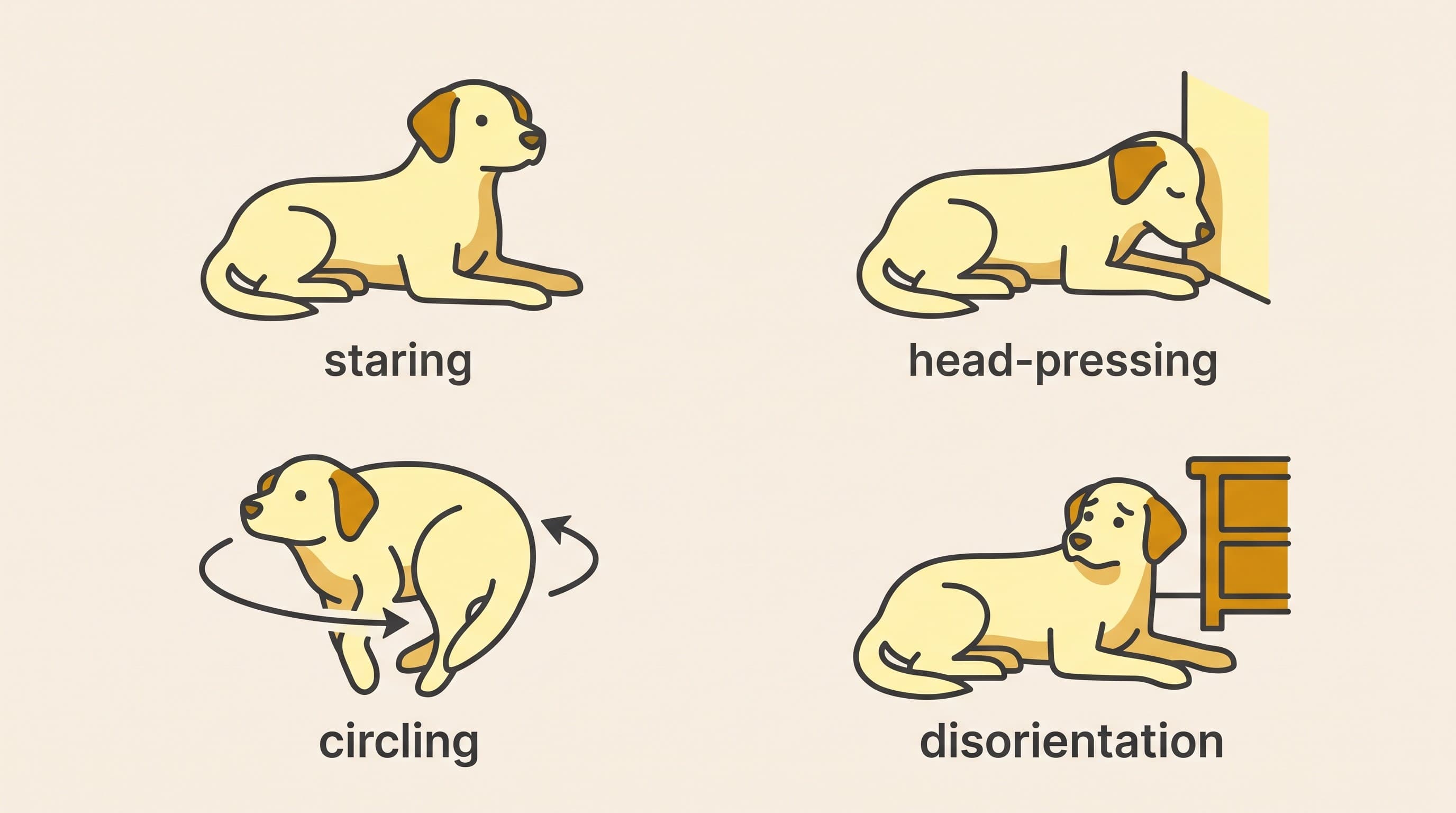
The signs are neurological and often subtle at first, which is part of why they are missed. Watch for:
- Staring into space or seeming vacant, as though the lights are on but nobody is home.
- Head-pressing, where your dog pushes the top of their head against a wall, a corner, or the floor and holds it there. This is an important and abnormal sign and always warrants a vet check.
- Circling or aimless pacing.
- Disorientation or confusion, not recognising you or the room, getting stuck in corners.
- Apparent blindness, walking into things they would normally avoid.
- Drooling or excessive salivation.
- Behaviour changes, sudden dullness, unusual quietness, or occasionally aggression.
- Seizures, at the more severe end.
Add to that the pattern: signs that fluctuate, that are often worse after eating, and in a dog who may also be small for their age, a poor grower, or slow to recover from anaesthesia (all clues that point at a shunt). No single sign is proof, but the combination, especially with a known or suspected liver problem, is what should make you and your vet think of HE rather than something purely neurological.
Why it gets mistaken for epilepsy, and why that matters
This is the heart of the piece, so let us be clear about it. A dog having a hepatic encephalopathic episode can look very much like a dog having a seizure or a post-seizure confused phase: the staring, the disorientation, the pacing, and in severe cases actual seizures. It is completely understandable that owners, and sometimes first-opinion vets, reach for "epilepsy" first, because epilepsy is common and HE is not something most people have heard of.
The reason the distinction matters is that the treatments are different. Epilepsy is managed primarily with anti-seizure medication. Hepatic encephalopathy is not, or at least not primarily. HE is treated by reducing the toxins reaching the brain and, where possible, by addressing the underlying liver problem. That usually means:
- Lactulose, which changes the gut environment so less ammonia is absorbed.
- Antibiotics, to reduce the ammonia-producing bacteria in the gut.
- Protein moderation, feeding the right amount of highly digestible protein rather than a big load that generates ammonia. Note: moderated, not eliminated. A protein-free diet is not safer and does its own harm.
- Addressing the shunt itself where that is an option, medically or surgically.
Treating true HE as though it were epilepsy, with anti-seizure drugs alone, misses the actual problem. That does not mean anti-seizure medication is never used in a liver dog; sometimes it is, on veterinary advice, to control seizures in the short term. But it is part of a bigger plan aimed at the liver and the toxins, not the whole answer. If your dog has been labelled epileptic and the picture does not quite fit, especially if the episodes cluster after meals or your dog is young and small, it is entirely reasonable to ask your vet, "could this be a liver problem?" and to ask about a bile acids test. You can read about that test and what it shows in the dedicated piece.
If you already know your dog has epilepsy and want to understand seizures in their own right, our epilepsy space covers that in depth (/spaces/condition-epilepsy). The point here is simply that the two can look alike, and in a dog with a liver problem, HE needs to be on the list.
An encephalopathic crisis is an emergency. If your dog becomes very dull or unresponsive, starts having repeated or prolonged seizures, becomes stuporous or collapses, or is head-pressing and disoriented and getting worse, this is a veterinary emergency. Do not wait to see if it passes and do not simply give an extra dose of a home medication and hope. Ring your vet or the nearest emergency service now and tell them your dog has a liver problem or a shunt. Untreated, a severe episode can be life-threatening.
What you can do at home, and what you can't
Between episodes, the mainstay is sticking faithfully to the plan your vet has set: the lactulose at the right dose, the antibiotics if prescribed, and the diet. Consistency genuinely matters here, because HE is driven by toxin levels and a missed dose or an off-plan meal can be enough to trigger an episode.
It is worth learning your dog's triggers, because HE episodes usually have one. The common ones are:
- A large protein-rich meal, which generates a surge of ammonia a few hours later. This is why the diet is moderated and why episodes so often follow dinner.
- Constipation, which lets more ammonia be absorbed from the gut the longer waste sits there.
- Dehydration, which concentrates toxins and stresses the system.
- Bleeding into the gut, for example from a stomach ulcer, because digested blood is a large protein load.
- Infections or any other new illness that upsets the balance.
- Certain medications and, in some dogs, the wrong dose of the wrong drug, which is one more reason all medication changes go through your vet.
Knowing this list helps you keep things steady, and it helps you recognise early when something is brewing. If your dog has been constipated or has picked up an infection and then starts seeming vacant, those dots are worth joining and mentioning to your vet, because dealing with the trigger is often part of settling the episode.
Lactulose has a useful double action here worth understanding: as well as reducing ammonia absorption, it loosens the stool, which helps counter the constipation that can itself trigger episodes. That is why your vet may adjust the lactulose dose to achieve soft, regular stools rather than to a fixed number on a syringe. Follow their guidance on this rather than guessing, because too little leaves the trigger in place and too much causes its own problems.
What you cannot do is manage a genuine crisis at home. Home care is for the stable, controlled phase. The moment your dog crosses into the territory in the red box above, this becomes a job for a vet, urgently. If you are ever unsure which side of that line your dog is on, treat it as the more serious one and call.
The bigger picture
Hepatic encephalopathy is frightening to witness, and the vacant, unreachable look on a dog you love is genuinely distressing. But it is also, in many cases, controllable. Dogs with shunts managed medically, and especially dogs whose shunts are corrected, can have their episodes greatly reduced or stopped altogether. The first step is recognising it for what it is rather than mislabelling it, because the right diagnosis leads to the right treatment.
If your dog has not yet had the liver side of things investigated, the bile acids test is usually where that starts, and it is worth reading about next. If a shunt has been found, the pieces on the surgery-versus-medical decision and on life after shunt surgery will help you understand where the treatment of the underlying cause can go. And keep the red box in mind: between episodes you are the steady hand on the routine, but a crisis belongs to your vet, straight away.
References
- Webster CRL, et al. ACVIM consensus statement on the diagnosis and treatment of chronic hepatitis in dogs. *J Vet Intern Med* 2019;33(3):1173–1200.
Keep track of how your pet is doing
The owners who cope best are the ones who notice changes early. A simple health log shows you what is working, and what is not, before the next vet visit.
Start tracking, freeYou're not doing this alone
Compare treatment journeys and talk to owners managing liver & gallbladder. Free to join.
Join PetsLikeMine